

Hepatocellular Carcinoma
Overview
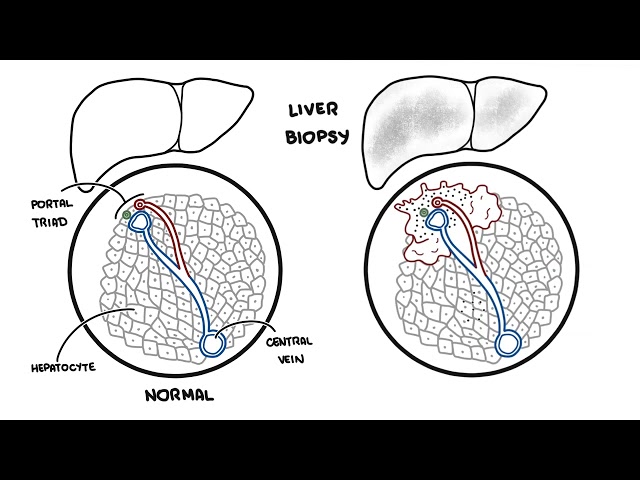
Hepatocellular carcinoma (also known as hepatoma ) is a primary cancer arising from hepatocytes in predominantly cirrhotic liver. Hepatocellular carcinoma is a leading cause of death worldwide, and cirrhosis is the main risk factor. Infection with hepatitis B and hepatitis C is the main cause of underlying liver disease. Prevention of chronic liver disease would greatly reduce incidence. Early tumour diagnosis through screening of at risk groups is cost effective.
Anatomy
The liver is wedge-shaped and is present in the right upper quadrant of the abdomen. The liver typically extends from the fifth intercostal space to the right costal margin in the midclavicular line.
| A normal liver that is palpable |
| In thin people |
| During deep inspiration |
| In the setting of a right pleural effusion |
| When emphysema results in hyperinflation of the chest with diaphragmatic descent and downward displacement of the liver |
Risk Factors
- Older Age
- Male gender
- Hepatitis B infection
- Hepatitis C infection
- Alfatoxins (mycotoxins – fungal) – Alfatoxin B1 is a potent carcinogen
- Non-alcoholic steatohepatitis (both independently and as a cofactor)
- Diabetes
- Family History of hepatocellular carcinoma
| Differential diagnosis of a Firm and Palpable Liver | History | Clinical Feature |
| Hepatocellular carcinoma | ||
| Metastatic Disease | ||
| Cirrhosis | ||
| Sarcoidosis | ||
| Hydatis disease | ||
| Differential Diagnosis of a Tender liver | History | Clinical Feature |
| Hepatitis | ||
| Budd-Chiari Syndrome (hepatic vein thrombosis) | ||
| Hepatocellular carcinoma | ||
| Hepatic abscess | ||
| Biliary Obstruction/chonlangitis |
| DIFFERENTIAL DIAGNOSIS OF A PALPABLE LIVER | ||
| Massive | Moderate | Mild |
| Metastasis | Massive causes | Massive and Moderate causes |
| Hepatocellular Cancer | Haemochromatosis | Hepatitis |
| Alcoholic liver disease | Haematological Disease | Biliary obstruction |
| Myeloproliferative disease | Secondary fatty liver disease (diabetes, obesity) | Hydatid disease |
| Right-sided heart failure | Amyloidosis | HIV infection |
Investigations & Diagnosis
General
Chronic liver disease screen
- Hepatitis B surface antigen
- Hepatitis C antibody
- Liver autoantibodies
- Immunoglobulins
- Ferritin
- alpha1-antitrypsin (also affects the lungs)
- Caeruloplasmin
Other investigations for Differential Diagnosis
- Amylase/lipase
- CEA
Screening with ultrasound for Hepatocellular carcinoma is recommended for patients with liver cirrhosis (as well as of other risk factors) every 6 months.
Classification
Child-Pugh Score (Determines liver function)
Barcelona clinic liver cancer (BCLC) staging classification – to help guide management – looks at the following factors:
- Performance status
- Child-Pugh score (determines liver function)
- Tumour size
- Multiple tumours
- Vascular invasion
- Nodal spread and extrahepatic metastases
| Barcelona clinic liver cancer | Feature |
| Stage 0 (very early stage) | Asymptomatic early tumours |
| Stage A (early stage) | Asymptomatic early tumours |
| Stage B (intermediate stage) | Asymptomatic multinodular tumours |
| Stage C (advanced stage) | Symptomatic tumours and/or invasive tumours |
| Stage D (end-stage) | Symptomatic treatment |
Treatment
Barcelona clinic liver cancer (BCLC) staging classification – to help guide management – looks at the following factors:
- Performance status
- Child-Pugh score (determines liver function)
- Tumour size
- Multiple tumours
- Vascular invasion
- Nodal spread and extrahepatic metastases
| Barcelona clinic liver cancer | Feature | Treatment |
| Stage 0 (very early stage) | Asymptomatic early tumours | Resection |
| Stage A (early stage) | Asymptomatic early tumours | Resection, percutaneous ablation, transplantation |
| Stage B (intermediate stage) | Asymptomatic multinodular tumours | Intra-arterial therapies (chemoembolisation and radioembolisation) |
| Stage C (advanced stage) | Symptomatic tumours and/or invasive tumours | Sorafenib, phase II trial agents, or palliative treatments |
| Stage D (end-stage) | Symptomatic treatment |
Treatment
- Resection
- Transplantation
- Percutaneous treatment
- Percutaneous ethanol injection
- Radiofrequency ablation
- Arterial embolization
- Sorafenib
Pharmacology
Sorafenib is indicated for the treatment of unresectable hepatocellular carcinoma and advanced renal cell carcinoma. It is a multikinase inhibitor, by inhibiting these kinases, genetic transcription involving cell proliferation and angiogenesis is inhibited. Sorafenib has been shown to prolong survival and is regarded as the standard of care. The adverse reactions observed at this dose were primarily diarrhoea and dermatologic events.
Complication & Prognosis
Complication
- Biliary obstruction
- Cachexia
- Hypoglycemia
- Hepatic failure
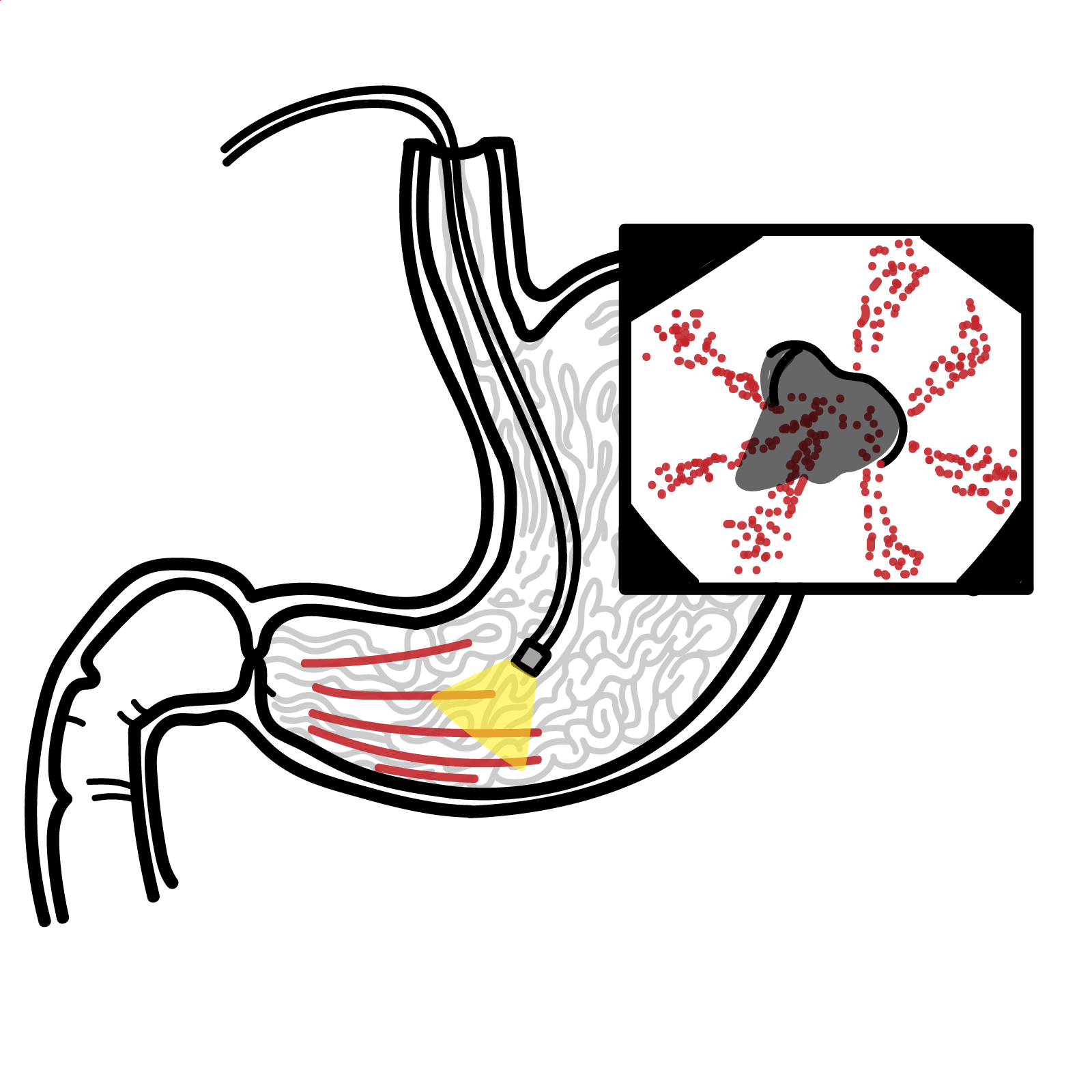
- Varicose veins
- Hepatic encephalopathy
- Ascites
- Peritonitis
- Hepatrenal syndrome
- Watery diarrhoea
- Paraneoplastic syndrome – Hypercalcaemia
- Intraperitoneal bleeding due to tumour rupture
Hepatoma is a very aggressive tumour. The clinical course and survival depends upon the stage and overall functional status of the liver
| Barcelona clinic liver cancer | Feature | Prognosis |
| Stage 0 (very early stage) | Asymptomatic early tumours | – |
| Stage A (early stage) | Asymptomatic early tumours | 50-70% 5 year survival with treatment |
| Stage B (intermediate stage) | Asymptomatic multinodular tumours | 50% 3 year survivial without treatment |
| Stage C (advanced stage) | Symptomatic tumours and/or invasive tumours | 50% 6 month survival |
| Stage D (end-stage) | Symptomatic treatment | 50% <3month survival |
References
BestPractice





Members only discussions coming soon…