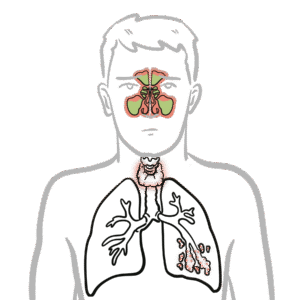
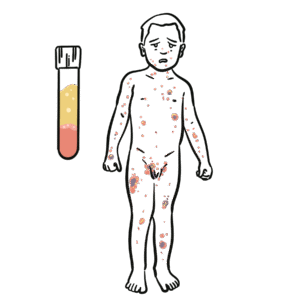
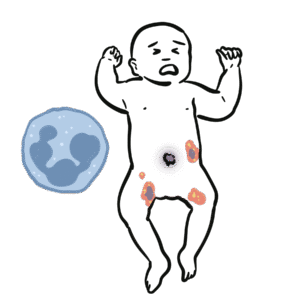
X-linked agammaglobulinaemia (XLA) is a rare primary immunodeficiency caused by mutations in the Bruton’s tyrosine kinase (BTK) gene, leading to failure of B-cell maturation. It results in profound hypogammaglobulinaemia and susceptibility to recurrent bacterial infections, particularly with encapsulated organisms. It usually presents after 6 months of age (once maternal IgG wanes). Prevalence is ~1 in 200,000 live male births.
Triad “Bruton’s = Boys, B-cells, Bacteria.”
Definition
BTK (Bruton’s tyrosine kinase): Enzyme critical for B-cell maturation. Hypogammaglobulinaemia: Low levels of immunoglobulins (IgG, IgA, IgM). Encapsulated bacteria: Bacteria such as S. pneumoniae, H. influenzae that require opsonising antibodies for clearance. Opsonisation: Process where antibodies coat bacteria to promote phagocytosis.
Anatomy & Physiology
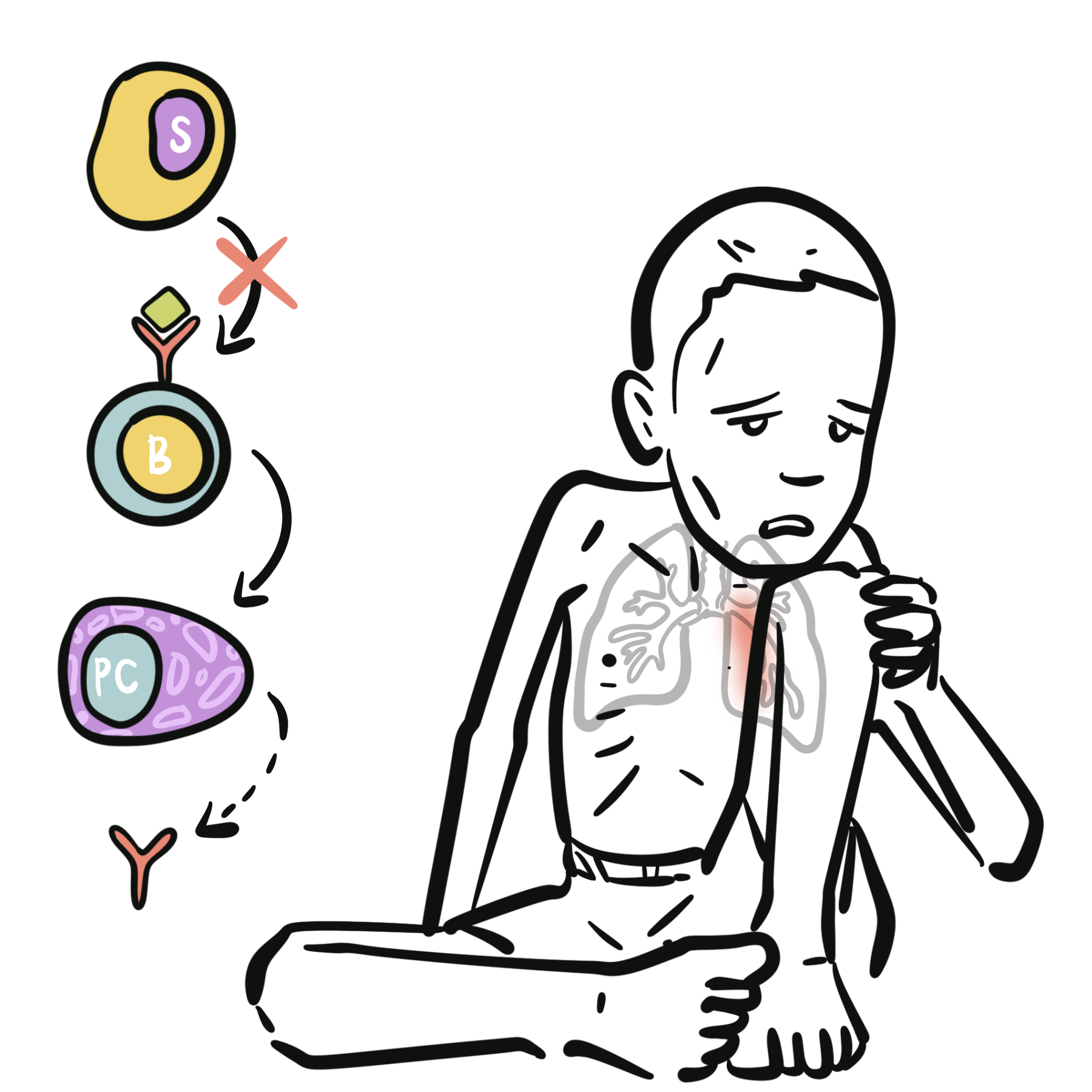
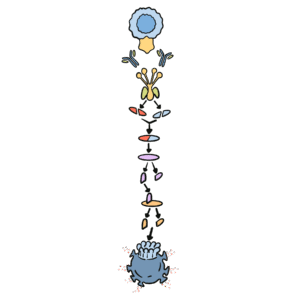
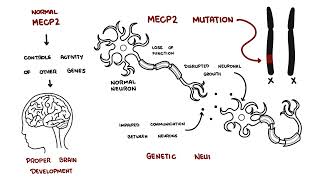
Normal B-cell development: Pro-B cell → pre-B cell (BTK required) → immature B cell → plasma cell producing antibodies.
In XLA, mutation in BTK halts differentiation at the pre-B stage, leading to:
Conley ME, Dobbs AK, Quintana AM, et al. Genetic basis of X-linked agammaglobulinemia. N Engl J Med. 2009;360(7):676–81.
Winkelstein JA, Marino MC, Lederman HM, et al. X-linked agammaglobulinemia: report on a United States registry of 201 patients. Medicine (Baltimore). 2006;85(4):193–202.
Ochs HD, Smith CIE. X-linked agammaglobulinemia: a model primary immunodeficiency. J Allergy Clin Immunol. 1996;98(4):687–99.
Picard C, Al-Herz W, Bousfiha A, et al. Primary immunodeficiency diseases: 2015 IUIS classification. J Clin Immunol. 2015;35(8):696–726.






Discussion