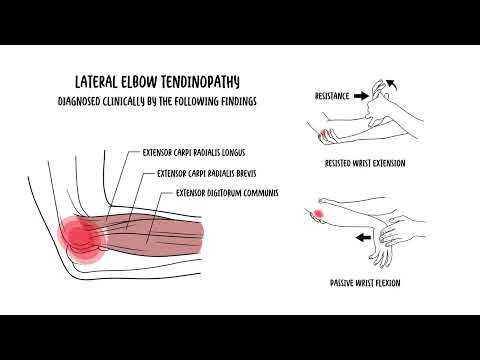
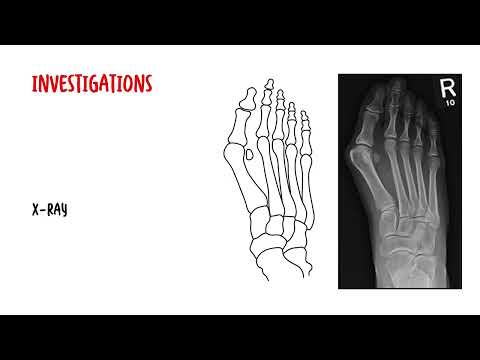
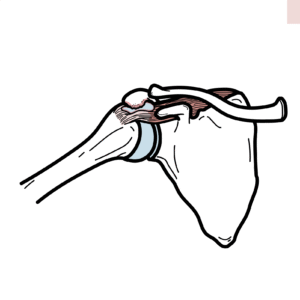
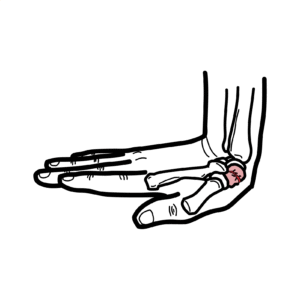
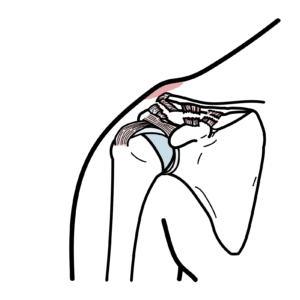
0:00 Medial elbow tendinopathy, also known as golfer's elbow, involves tendinosis at 0:17 the common origin 0:18 of the flexor pronata muscle groups, typically caused by repetitive flexion and 0:23 pronation 0:24 of the wrist. 0:25 It is frequently observed in athletes involved in throwing sports, racket 0:30 sports, and golf. 0:32 Those affected by this condition often experience inner elbow pain that worsens 0:35 during activities 0:36 such as throwing, serving, or hitting a forehand. 0:40 Additionally, symptoms may include a weak grip and peristhesias in the ring and 0:45 little 0:46 finger, which could indicate an ulna neuropathy. 0:55 Let's revise some anatomy. 0:57 The distal humerus has a medial and lateral epicondyle. 1:02 The epicondyle's are bony promenances easily palpated on the medial and lateral 1:07 sides 1:07 of the distal humerus, just proximal to the elbow joint. 1:12 The lateral humerus epicondyle serves as the bony common origin of the wrist 1:18 and extrinsic 1:19 hand extensors. 1:21 This is where the extensors of the hands originate, whereas the medial humerus 1:26 epicondyle serves 1:28 as the bony common origin of the wrist and extrinsic hand flexors. 1:32 These are where the hand flexors originate, the medial epicondyle. 1:42 So medial elbow tendinopathy is essentially irritation or tendinosis of the 1:47 medial epicondyle 1:50 where the tendons insert. 1:52 It is diagnosed clinically by the following findings. 1:55 Localized tendinists over the medial epicondyle and proximal wrist flexor 2:01 muscle mass, pain 2:03 with resisted wrist flexion and pronation with the elbow in full extension, 2:11 pain with 2:12 passive wrist extension with the elbow in full extension. 2:18 So what's the difference between medial and lateral elbow tendinopathy? 2:27 Well, as the name suggests, medial elbow tendinopathy or golfer's elbow affects 2:31 the inner elbow 2:32 and is associated with the flexor pronator muscle group, leading to pain 2:37 exacerbated 2:38 by movements such as wrist flexion and pronation. 2:43 Conversely, lateral or outer elbow tendinopathy, known as tennis elbow, impacts 2:49 the outer elbow 2:50 and involves the extensor muscles, particularly the extensor copy radialis bre 2:57 vis. 2:58 One in lateral elbow tendinopathy typically worsens with wrist extension and 3:04 supination 3:04 movements. 3:12 Investigations for medial elbow tendinopathy while imaging tests such as x-rays 3:16 , ultrasounds 3:16 and MRIs are not routinely performed but can be useful. 3:20 Typically x-rays do not show abnormalities, whereas ultrasound might reveal 3:24 decreased 3:24 echogenicity, inhomogeneity and thickening of the tendons, sometimes 3:29 accompanied by 3:30 a local fluid collection. 3:33 MRIs can show increased signal intensity near the medial epicondyle. 3:43 Treatment of medial elbow tendinopathy generally begins with non-operative 3:47 methods, of course, 3:49 including rest, application of ice, if it's acute, 10-20 minutes every few 3:55 hours during 3:56 acute stages, compression later on, and the use of topical non-stronal anti- 4:01 inflammatory 4:02 drugs such as Voltaire and Gel, or oral anti-inflammatory drugs. 4:07 If these conservative approaches fail, a treatment plan might include an 4:11 injection of corticosteroid. 4:14 It's crucial to limit the amount of injections given for tendinopathy, as there 4:20 could be 4:21 associated tendon damage and even complications to the ulnar nerve, which runs 4:25 quite close 4:26 to this area. 4:33 If symptoms persist despite adequate conservative treatment, surgical 4:37 intervention may be considered. 4:39 Insurgical treatment might involve releasing the flexor or pronata origin, 4:45 removing granulation 4:47 tissue, de-cordicating the medial epicondyle bone, and reconstructing the 4:54 medial musculo-tendinous 4:56 unit. 5:03 In summary, we looked at medial elbow tendinopathy, also known as golfers elbow 5:08 , which 5:09 involves tendinosis at the common origin of the flexor-pronata muscle group. 5:16 It's typically seen in people who do repetitive flexion and pronation of the 5:20 wrist, such 5:20 as in golf, or any throwing sports. 5:24 Treatment includes conservative, corticosteroid injection, and very rarely 5:29 surgery. 5:30 Thank you for watching. 5:39 �