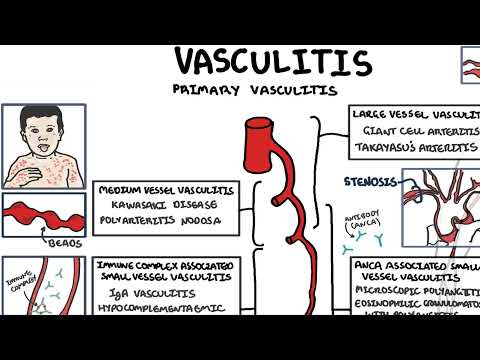
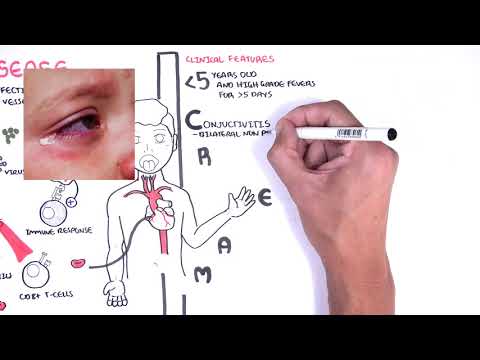
0:00 Hello, in this video we're going to talk about medium vessel vasculitis. 0:12 Vasculitis is inflammation of the blood vessels resulting in damaged vessels 0:16 which can lead 0:17 to potential complications such as organ ischemia as well as aneurysms. 0:25 Many vasculidides are classified into the size of the blood vessels affected. 0:31 Large vessel vasculitis, medium vessel vasculitis and small vessel vasculitis. 0:37 The medium vessel vasculitis includes poly-autritus nodosa and Kawasaki disease 0:46 . 0:46 Poly-autritus nodosa is a rare systemic necrotizing vasculitis, targeting 0:51 medium-sized arteries. 0:55 Poly-autritus nodosa has distinct features with particular involvement of the 1:00 renal 1:00 and visceral arteries. 1:02 It is associated with hepatitis B, virus, mononuritis multiplex, and renal inf 1:09 arction. 1:10 There is no involvement of the lungs, ecynophils are usually normal, and there 1:15 is absence of 1:16 anti-neutrophilic cytoplasmic antibodies. 1:22 The meaning of poly-autritus nodosa is characterized by focal and segmental, 1:26 transmural necrotizing 1:28 inflammation, which is essentially inflammation on all the layers of the blood 1:33 vessel, a pan-artritus. 1:36 The exact etiology is unknown, but possibly infection, and because of its 1:41 association 1:42 with hepatitis B virus, this could be the potential trigger. 1:46 From whatever antigen, an antigen-presenting cell can activate T-cells, which 1:49 will in turn 1:51 stimulate the immune response. 1:53 In poly-autritus nodosa, likely the cell-mediated immune response is stimulated 1:58 , which involve 1:59 the macrophages and the neutrophils. 2:02 In the acute phase of the disease, neutrophils infiltrate all layers of the 2:06 blood vessels, 2:07 causing damage to the surrounding tissue. 2:11 Macrophages will then move in to clean up the area. 2:15 The impairment of the vessel wall begins, is platelet plug formation as well as 2:20 fibrin deposition. 2:24 Collagen gets deposited as the vessel is repaired. 2:27 The segment of blood vessels here become fibrosed. 2:32 This area is now termed fibrenoid necrosis, which is a special histopath 2:37 ological term 2:38 seen in blood vessel necrosis. 2:42 And this is where segmental, transmural, necrotizing inflammation comes in. 2:48 There is necrosis of the blood vessel in segments. 2:55 Fibrenoid necrosis include dead cells and dead immune cells, collagen, proteins 3:01 and 3:01 fibrin. 3:03 The vessel is now not as strong, aneurysms can occur. 3:07 These are dilatations of up to 1 centimetre in size along the involved arteries 3:13 . 3:13 And this is characteristic of polyiotratus nodosa. 3:17 At a macroscopic view, blood vessels look like beads on a string. 3:24 Polyiotratus nodosa commonly involves bifurcation and branching of the arteries 3:32 . 3:33 During the healing process, lumen narrowing can occur thanks to a number of 3:37 factors through 3:37 thrombosis and fibren deposition, collagen deposition and hypertrophy of the 3:43 smooth muscle 3:44 layers. 3:48 The association with hepatitis B virus is because patients with hepatitis B can 3:54 often 3:54 present with polyiotratus nodosa. 3:57 So what is the clinical features of polyiotratus nodosa? 4:01 Clinical features of polyiotratus nodosa are nonspecific symptoms such as fe 4:05 vers, myalgia, 4:06 weight loss and a rash. 4:08 Nervous system involvement is common with peripheral neuropathy and mononuritis 4:14 multiplex being 4:15 the most common. 4:17 Mononuritis multiplex, also called multiple mononuropathy, refers to an 4:22 anatomical pattern 4:23 of peripheral neuropathy that affects two or more different nerves basically. 4:29 It's thought to be due to inflammation and occlusion of the vaso-nervorum, the 4:34 blood 4:35 vessel that actually supplies the nerves. 4:42 Another feature of polyiotratus nodosa is the involvement of the renal artery 4:46 which can 4:47 lead to renal infarction and this is just due to inflammation of the blood 4:51 vessel. 4:52 Also, the renal artery involved can lead to hypertension, secondary to the ren 4:58 in angiotensin 4:59 aldosterone system being activated. 5:04 Important to mention that the risk of cardiovascular morbidity and mortality is 5:09 high in polyiotratus 5:11 nodosa and requires close monitoring. 5:14 The rash in polyiotratus nodosa can be numerous things including a perperic 5:20 rash, subcutaneous 5:22 nodules, bullets of vesticular lesions and levido reticularis. 5:33 There is also GI involvement characterized by nonspecific abdominal pain in up 5:38 to 50% 5:38 of cases. 5:43 The investigations to order for someone suspected of polyiotratus nodosa 5:48 includes a viral hepatitis 5:50 serology, full blood count and EUCs, electrolyte urea creatinine to check renal 5:57 function. 5:58 Diagnosis of polyiotratus nodosa is through a biopsy but in the absence of an 6:03 easily accessible 6:04 tissue for biopsy, the arteriographic demonstration of involved vessels 6:10 particularly in the form 6:12 of aneurysms of the small and medium-sized arteries in the renal hepatic and 6:16 visceral 6:17 vascular literature is sufficient to make the diagnosis. 6:23 Here is an image of an angiogram showing the renal artery supply. 6:27 Note the small aneurysms throughout the medium-sized vessels. 6:35 The classic polyiotratus nodosa should be treated with a combination of 6:39 steroids, glucocorticoids 6:41 and cyclophosphamide. 6:44 The treatment of hepatitis B virus-associated polyiotratus nodosa involves a 6:49 different 6:49 approach. 6:52 Prognosis of untreated patients is poor and mainly due to gastrointestinal 6:57 complications 6:58 and cardiovascular complications mentioned earlier. 7:02 Important to know about another condition called cutaneous polyiotratus nodosa. 7:08 Whereas classic systemic polyiotratus nodosa commonly affects the kidneys, 7:12 muscles, nerves 7:14 and GI tract as well as the skin, vasculitis is skin limited. 7:29 The other type of medium-sized vasculitis is Kawasaki disease. 7:33 Kawasaki disease is an uncommon systemic vasculitis disease affecting mainly 7:38 children under the 7:39 age of 5. 7:41 Kawasaki disease is a medium-sized vasculitis. 7:45 Kawasaki disease and Hinokshanland perpera are the most common, primary vascul 7:50 ities in 7:50 children. 7:51 It is more prevalent in Asians and native Pacific Islanders and is a leading 7:56 cause of 7:57 childhood acquired heart disease in developed countries, which include coronary 8:03 aneurysms. 8:04 The exact cause of Kawasaki diseases are known, but clinical and epidem 8:08 iological data support 8:10 infectious cause. 8:12 In Kawasaki disease, an intense inflammatory cell response develops in a wide 8:17 array of 8:18 organs and tissues in medium-sized arteries such as the coronary arteries. 8:25 The pathophysiology of Kawasaki involves monocytes, IgA antibodies, neutrophils 8:32 in the acute setting 8:34 and cytotoxic T cells. 8:36 These guys all play a role in the inflammation of the medium-sized vessel. 8:41 What is thought to drive this temporary vasculitis is an infection. 8:46 Theories include staphylococcus and streptococcus species such as from strep 8:52 throat and even 8:53 a viral infection. 8:57 Antigen presenting cells will pick up these antigens and mount an inflammatory 9:01 response. 9:02 The inflammatory response somehow misdirects the attack and will attack the 9:06 medium-sized 9:07 vessels temporarily and this includes the coronary arteries. 9:13 This response can damage collagen and damage elastic fibres in the vessel walls 9:19 and can 9:19 lead to loss of their normal structural integrity. 9:25 Despite the repair that occurs, the disrupted structural integrity results in 9:29 ballooning 9:30 or aneurysm formation. 9:35 The clinical features of Kawasaki is usually a child less than 5 years old with 9:40 high fevers 9:41 for more than 5 days and irritability. 9:46 Some classic findings in Kawasaki can be remembered with the abbreviation cream 9:53 . 9:53 D is for conjunctivitis, bilateral non-paralint. 10:00 R is for rash, polymorphous or macular papular rash. 10:08 E is for erythema and/or edema of the hands or feet. 10:17 A is for adenopathy, lymph adenopathy specific with a cervical chains. 10:24 And M is for mucous membrane changes which include red tongue, strawberry 10:29 tongue and 10:30 dry cracked lips. 10:34 The diagnosis of Kawasaki is made if the child has 4 of the 5 following letters 10:41 in cream 10:43 as well as having a fever for more than 5 days. 10:48 For children who present with a perpera or a particular rash with fever, the 10:51 differential 10:52 is broad. 10:53 A good start is to divide differentials into thrombocytopenia and non-thrombocy 10:59 topenia 11:00 induced rash. 11:02 But some important differential diagnosis to remember include measles, where 11:07 there is 11:07 evidence of exudative conjunctivitis, coplic spots and rash which tend to occur 11:12 in the 11:12 head and migrate to the trunk. 11:15 Drug reaction is important differential which leads to a generalized rash 11:18 eruption all over 11:19 the body, usually itchy and another important feature is the angioedema which 11:26 is swelling. 11:27 Infections is a fundamental differential and includes streptococcus infections. 11:32 And remember, infections are associated with the development of Kawasaki. 11:37 So for example streptococcus pharyngitis and streptococcus pharyngitis can then 11:43 also 11:43 lead to scarlet fever, streptococcus pharyngitis can also lead to rheumatic 11:47 fever and autoimmune 11:48 response to the streptococcus infection. 11:52 Another differential are the staphylococcus infections, which typically include 11:55 the skin 11:57 and is also associated with the development of Kawasaki disease. 12:01 Staphylococcus infection differentials include staphylococcus scarlet skin 12:06 syndrome, which 12:07 is characterized by red blistering skin that looks like a burn. 12:13 Another is toxic shock syndrome which is caused by the release of bacterial 12:19 toxins from the 12:20 staphylococcus species and is associated with tampon use. 12:26 Another important differential and also potentially the trigger for Kawasaki 12:29 are viral infections 12:30 which can also manifest as a macular papular rash. 12:33 Finally, a very life threatening differential is Stephen Johnson syndrome. 12:41 Investigations to order include a full blood count to look for signs of 12:44 infection, EUCs 12:46 for kidney involvement, LFTs to look for viral causes affecting the liver, CRP 12:51 and ESR which 12:51 are inflammatory markers, these should be high in Kawasaki as well as in 12:58 infections. 12:59 Another analysis is good to look for evidence of an increase in white cell 13:03 count. 13:04 Finally, it is suggested that an echocardiogram should be performed once the 13:08 diagnosis of 13:09 Kawasaki disease is made as well as 6-10 weeks after to check for myocardial 13:16 inflammation 13:16 and coronary artery aneurysm formation. 13:20 Remember, the main complication of Kawasaki disease is coronary artery aneurysm 13:26 , but it 13:26 is not uncommon for aneurysms to occur anywhere along the branches of the aorta 13:33 . 13:33 Once diagnosis of Kawasaki is made, it is essential that a pediatrician is 13:38 involved. 13:39 Admit the child and commence immunoglobulin intravenously as well as aspirin. 13:46 Commencing intravenous immunoglobulin within 10 days of fever onset has shown 13:50 to reduce 13:50 cardiac complications. 13:53 The complications of Kawasaki are mainly cardiovascular and include coronary 13:58 artery aneurysms as well 14:00 as artery aneurysms anywhere else, myocardial infarction, pericarditis and my 14:07 ositis. 14:08 Thank you for watching, that concludes the video on medium-sized vessel vascul 14:15 itis. 14:23 You