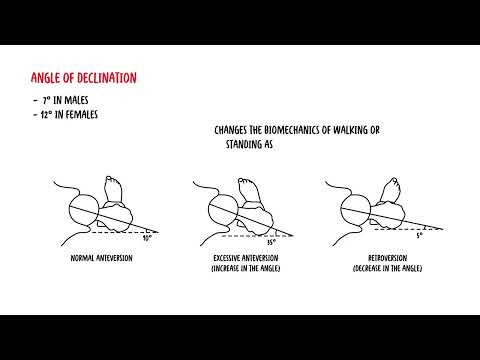
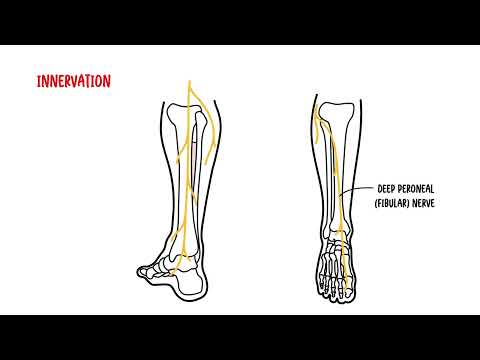
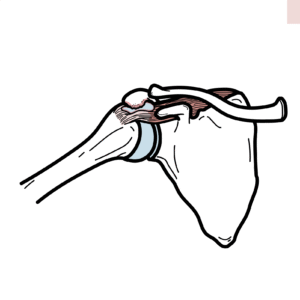
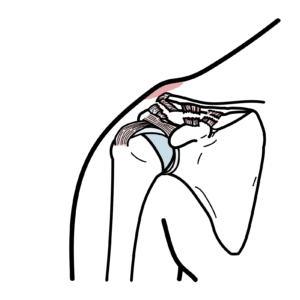
0:00 The shoulder joint is also known as the glenohumoral joint. 0:15 It is a synovial joint that attaches the upper limb to the axial skeleton. 0:21 The shoulder joint is a ball and socket joint. 0:25 It is formed by the articulation of the head of the humerus and the glenoid 0:30 cavity, also 0:31 known as the glenoid fossa. 0:34 The glenoid cavity or glenoid fossa is part of the scapula. 0:39 The articulating surfaces of the joint are covered with highline cartilage. 0:49 The shoulder joint is the most mobile joint of the human body. 0:53 It allows for a wide range of movement at the upper limb. 0:59 Flexion, extension, abduction, adduction, internal and external rotation, and 1:10 circumduction. 1:13 However, this mobility comes at a cost of stability, as its bony surface offer 1:22 little 1:22 support. 1:24 The shoulder joint is instead surrounded by muscles and ligament structures 1:27 that offer 1:28 the joint security. 1:30 Due to this, the shoulder joint is actually one of the most frequently disl 1:35 ocated injured 1:36 joints in the body. 1:43 Let's first begin by talking about components of the shoulder joint, beginning 1:48 with the joint 1:48 capsule. 1:50 The joint capsule is a fibrous sheath that encloses the structures of the 1:54 shoulder joint. 1:57 Here is a coronal section of the right shoulder joint, as we look at it 2:02 straight on. 2:04 The synovial membrane lines the inner part of the joint capsule and produces 2:11 synovial 2:12 fluid to reduce friction between the articular surfaces. 2:17 That is why the shoulder joint is a synovial joint. 2:21 The outer part of the capsule contains parts of the ligaments, of the shoulder 2:26 as well 2:26 as muscles. 2:30 Now, there are several ligaments that stabilizes the shoulders. 2:39 There is the glenohumoral ligaments, which is composed of the superior, middle 2:45 and inferior 2:45 parts. 2:47 And the glenohumoral ligament extends from the humerus to the glenoid fossa, 2:53 and acts 2:53 to reinforce the joint capsule. 2:56 The glenohumoral ligaments act to stabilize the anterior aspect of the joint. 3:05 The chorocohumoral ligament extends from the base of the chorocoid process to 3:09 the greater 3:10 tubercle of the humerus. 3:14 This ligament supports the superior part of the joint capsule. 3:18 Next, the transverse humoral ligament is found between the two tubercles of the 3:23 humerus. 3:24 The biceps tendon runs through here. 3:29 The chorocohomial ligament extends from the choromian and chorocoid process of 3:34 the scapula, 3:35 and forms an arch-like structure found over the shoulder joint. 3:40 This is referred to as the chorocohocromial arch. 3:45 This ligament acts to resist superior dislocation of the head of the humerus. 3:52 Next, let's talk about some important muscles that help stabilize the shoulder 4:00 joint. 4:01 And these are called the rotator cuffs. 4:05 The rotator cuffs are composed of tendons of four muscles. 4:10 The subscapularis is located anteriorly on the scapula. 4:18 The supraspinatus, infraspinatus, and terrace minor are located posteriorly on 4:24 the scapula. 4:25 The supraspinatus comes over the top here, as you can see. 4:30 These muscles and tendons provide stability in the shoulder, attaching around 4:36 the head 4:37 of the humerus bone, encircling it like a cuff. 4:41 The primary function of the rotator cuff is to position the humeral head in the 4:46 glenoid, 4:46 allowing the larger muscles to provide necessary power. 4:55 Next, talking about the bursa, the shoulder joint has several bursa, which acts 5:01 as a cushion 5:02 between tendons and other joint structures. 5:06 There are two main bursas found in the shoulder. 5:08 Firstly, the subacromial bursa, which is located deep in the deltoid and acrom 5:14 ion, and superficial 5:16 to the supraspinatus tendon and joint capsule. 5:20 It acts to reduce friction under the deltoid, which enables free motion of the 5:26 rotator 5:27 cuff tendons. 5:29 Secondly, you have the subscapula bursa, and this is found between the subscap 5:34 ularis 5:34 tendon and the scapula. 5:36 It acts to reduce friction on the tendon during movement of the shoulder joint. 5:47 The blood supply to the shoulder joint is provided by the anterior and 5:51 posterior circumflex 5:53 humeral arteries. 5:55 These are both branches of the auxiliary artery. 5:59 There are also contributions from the supra scapula artery, which is a branch 6:04 of the thyroid 6:05 cervical trunk. 6:08 And this brings us to innovation. 6:15 The sensory innovation to the area is really by the auxiliary and supra scapula 6:24 nerves. 6:25 These nerves are also responsible for motor function of some of the muscles 6:30 that we have 6:31 learned. 6:33 So here you can see the auxiliary nerve next to the auxiliary artery and the 6:39 supra scapula 6:41 nerve next to the supra scapula artery. 6:46 And as you can see, these innervate some associated muscles we have already 6:56 learned. 6:58 Some clinical anatomy. 6:59 Now, we will briefly talk about four clinical conditions that relate to the 7:05 shoulder joint 7:06 and brief examination findings. 7:09 First of all, beginning with rotator cuff tears. 7:13 Rotator cuff tears are the most common cause of shoulder pain. 7:17 And this is because the tendons of the rotator cuff are often under a lot of 7:21 strain, as they 7:22 function in stabilizing the glenohumeral joint. 7:27 Rotator cuff tears occur when there is a complete separation of the tendinous 7:31 fibers from their 7:32 insertion onto the greater tuberosity of the humerus. 7:39 The clinical features include pain around the shoulder that may radiate down 7:43 the humerus. 7:44 Pain can be worse with overhead activity affecting day-to-day life and even 7:49 sleep. 7:49 Rotator cuff injuries will be discussed in more detail in a separate video. 7:59 Next clinical anatomy is a condition called shoulder impingement. 8:04 Heart impingement is a group of conditions that actually is where you have ent 8:09 rapment 8:09 of the musculoskeletal soft tissue within the shoulder and this most often 8:14 presents 8:14 in pain. 8:15 It is an overuse injury with compression of the rotator cuffs between the 8:20 greater tuberosity 8:21 of the humerus and the acromine. 8:24 Common presentation is usually where one develops pain that is gradual and may 8:29 present 8:30 for weeks or months around the shoulder area specifically in the lateral delto 8:35 in just distal 8:36 to the tip of the acromion. 8:37 Again, the pain is worse with overhead activity. 8:41 Commonly, you can even see local swelling and tendinous in the front of the 8:46 shoulder. 8:47 On examination, when someone abducts their arm between 90 and 120 degrees, they 8:56 can 8:57 develop pain and this is called the painful arc, so it is positive for a 9:02 painful arc 9:02 which can indicate a shoulder impingement. 9:06 Because again, the soft tissue structures here are impinged between the head of 9:11 the humerus 9:12 and the acromion. 9:20 The next clinical condition is shoulder dislocation and shoulder instability. 9:26 As said previously, the shoulder joint is one of the most frequently dislocated 9:29 joints 9:29 in the body. 9:31 Dislocations at the shoulder are described by where the humeral head lies in 9:36 relation 9:37 to the glenoid fossa. 9:38 95% of shoulder dislocations are anterior dislocations, however posterior and 9:44 inferior 9:45 dislocations can also occur, about 4% and 1% respectively. 9:51 Their displacement is prevented by the carocochromial arch. 10:02 The most common type of dislocation is anterior dislocation and it is a result 10:05 of excessive 10:06 extension and external rotation of the humerus. 10:12 In anterior dislocation, the humeral head is forced anteriorly and inferiorly 10:16 into the 10:17 weakest point of the joint capsule. 10:19 Now, if the joint capsule is torn, there is an increased risk of future disloc 10:25 ations. 10:26 Posterior dislocation is uncommon and it typically occurs in people who have 10:29 seizures 10:29 and electrocution injuries. 10:38 There are some complications of shoulder dislocations. 10:41 Now, the auxiliary nerve as we have learned is located very closer on this area 10:46 and it 10:47 can be damaged in the dislocation of the shoulder or even during attempted 10:51 reduction 10:52 of the shoulder. 10:54 And remember that the nerve runs in close proximity to the shoulder joint and 10:58 around 10:59 the surgical neck of the humerus. 11:02 If the auxiliary nerve is injured, paralysis of the deltoid occurs as well as 11:06 loss of sensation 11:07 over the regimental badge area, which is the inferior portion of the deltoid. 11:20 The last clinical condition to talk about is something called frozen shoulder, 11:24 also known 11:25 as adhesive capsulitis. 11:28 And interestingly enough, this occurs in approximately 2 to 5% of people. 11:33 It is characterized by initially painful and latter progressively restricted 11:38 active and 11:38 passive movements of the glenohumoral joint. 11:42 The cause of frozen shoulder is believed to be inflammation in the shoulder 11:48 capsule itself, 11:50 which causes pain and capsulofibrosis and adhesion, and this leads to decreased 11:56 range 11:56 of motion in all planes. 11:59 Pain is often gradual around the shoulder before any noticeable loss of motion. 12:05 This is then followed by pain at rest and then pain with movement in all 12:09 direction. 12:10 And so on examination, there is limitation in movement in both active and 12:14 passive movements, 12:16 especially in abduction of the shoulder, internal and external rotation. 12:21 These are very important findings to differentiate between other shoulder 12:25 problems. 12:26 Most factors for frozen shoulder include being female, increasing age and 12:35 having diabetes. 12:38 So in summary, today we talked about the clinical anatomy of the shoulder joint 12:42 . 12:42 We discussed the general anatomy of the shoulder joint, its vascular supply and 12:46 innovation. 12:47 We then discussed clinical cases relevant to the shoulder joint. 12:50 These are rotator cuff tears, shoulder impingement, shoulder dislocation and 12:55 stability and frozen 12:57 shoulder. 12:58 In a separate video we will focus more in depth of the rotator cuff muscles and 13:02 specific rotator 13:03 cuff injuries. 13:04 Thank you for watching. 13:20 [BLANK_AUDIO]