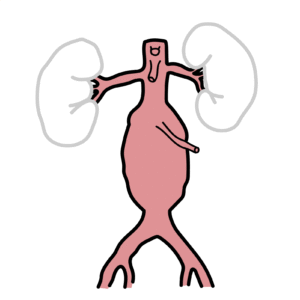
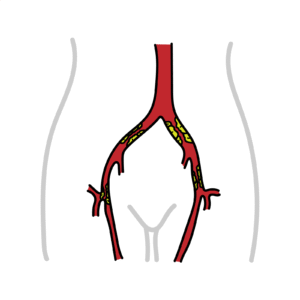
0:00 The superior mesenteric artery syndrome is a rare cause of small bowel 0:09 obstruction. 0:10 From compression of the third part of the duodenum, by the superior mesenteric 0:15 artery 0:15 anteriorly and the aorta or vertebra posteriorly. 0:20 The cause is usually from loss of mesenteric fat pad between the superior mes 0:25 enteric artery 0:26 and the aorta. 0:29 Let's revise some anatomy, so here we have the stomach and the duodenum, the 0:32 first part 0:32 of the small intestine, which is held by the ligament of treats. 0:38 The superior mesenteric artery arises from the anterior aspect of the aorta, at 0:43 the level 0:45 of the L1 vertebral body. 0:48 Above the superior mesenteric artery is a celiac artery, and below is the renal 0:52 artery, at about 0:53 L2. 0:57 The superior mesenteric artery goes over two important structures, the third 1:01 part of the 1:01 duodenum and the left renal vein that then drains into the inferior vena cava. 1:07 As the superior mesenteric artery arises from the aorta, it is surrounded by 1:11 fat allowing 1:12 it to extend at a particular angle between 28 to 65 degrees. 1:18 This angle is called the aortomyzenteric angle. 1:21 The aortomyzenteric distance is 10 to 34 millimeters. 1:31 The superior mesenteric artery supplies blood to the small intestine, basically 1:36 , the ascending 1:38 colon and the part of the or majority of the transverse colon. 1:42 Embryologically, these structures are called the mid-gut. 1:47 In superior mesenteric artery syndrome, what occurs is you have compression of 1:53 the duodenum 1:54 by the superior mesenteric artery against the aorta or the vertebra. 2:00 The aortomyzenteric angle is less than 25 degrees, and the aortomyzenteric 2:05 distance is 2:05 typically less than 8 millimeters. 2:08 Most common association is significant weight loss, leading to loss of the mes 2:13 enteric fat 2:14 pad, the yellow stuff here, and so reduced aortomyzenteric angle, compressing 2:19 the third 2:19 part of the duodenum, causing a small bowel obstruction. 2:24 So risk factors for developing superior mesenteric artery syndrome include 2:28 significant weight 2:29 loss, leading to loss of mesenteric fat pad as a consequence of any medical 2:34 disorders, 2:35 psychological problems, or surgery. 2:38 So for example, extreme weight loss can be from bariatric surgery, spinal cord 2:44 injury, 2:45 paraplegics, prolonged bed rest. 2:48 Spinal surgery can also cause this condition through a correction of scoliosis. 2:57 So what about the clinical features? 3:00 Well, superior mesenteric artery syndrome causes small bowel obstruction, which 3:04 can be acute 3:05 or gradual. 3:06 Symptoms include abdominal pain, nausea, vomiting, and loss of flatus. 3:13 Patients with mild obstruction may have only postprandial epigastric pain and 3:19 early satiety 3:21 with associated weight loss. 3:25 Symptoms may be relieved when patient is lying prone in a left lateral de-cubid 3:30 ous position 3:31 or in a knee chest position, like you're having a lumbar puncture. 3:36 These positions remove the tension from the mesenteric artery and superior mes 3:40 enteric artery 3:41 opening the space between the superior mesenteric artery and the aorta. 3:45 Findings on physical examination are nonspecific, but can include abdominal 3:49 distension if there's 3:50 a bowel obstruction, a succession splash, and a high-pitched bowel sound. 3:58 Another presentation of superior mesenteric artery syndrome could also include 4:03 when the 4:04 superior mesenteric artery compresses the left renal vein, which normally 4:07 drains into the 4:08 inferior vena cava. 4:10 The left renal vein compression can affect the left testicular vein, which 4:14 normally drains 4:14 into the left renal vein. 4:17 This will cause compression, congestion in the renal vein, the left testicular 4:21 vein causing 4:21 what's called a varicoseal, which is a painful testicular enlargement due to 4:26 congestion of 4:27 the venous plexus here. 4:29 When the superior mesenteric artery compresses the left renal vein causing a 4:33 varicoseal, 4:34 this condition is termed the nutcracker syndrome. 4:37 Of course, the varicoseal is typically the left side because the right test 4:42 icular vein 4:42 drains straight into the inferior vena cava. 4:51 Diagnosis of superior mesenteric artery syndrome can be challenging, and it is 4:56 uncommon with 4:57 nonspecific symptoms. 4:59 However, oral contrast can be used. 5:02 So these are upper gastrointestinal series, which usually demonstrate delay and 5:08 passage 5:09 of the contrast from the duodenum to the next part of the small intestine. 5:16 Imaging of the arterial system can also help with contrast through CT or MR. 5:25 Treatment can be divided into conservative or surgical. 5:30 Conservative, really because weight loss is a big risk factor, weight gain is 5:36 recommended. 5:37 If bowel obstruction occurs, gastrointestinal decompression with a nasogastric 5:42 tube is important 5:43 as well as correction of electrolyte abnormalities. 5:46 In terms of surgery, if the condition is not improving with conservative 5:50 management, there 5:51 are three major surgical options. 5:53 These are the strong procedure where you have mobilization of the ligament of 5:58 treats, allowing 5:58 the displacement of the duodenum. 6:03 There's gastro-juginostomy, which is basically when the gastric or the stomach 6:07 is connected 6:08 to the juginum, the second part of the small intestine, or even better, a duod 6:15 enum duodenostomy, 6:17 which is where the duodenum is actually connected to the juginum, but more prox 6:23 imal the juginum 6:24 is connected to the juginum. 6:29 So in summary, superior mesenteric artery syndrome is a very rare cause of 6:32 small bowel 6:32 obstruction caused by compression of the third part of the duodenum by the 6:36 superior mesenteric 6:37 artery. 6:38 It is associated with significant weight loss and treatment can be broadly 6:41 divided into 6:41 conservative or surgical management. 6:43 Thank you for watching.