

Anal Haemorrhoids

Overview
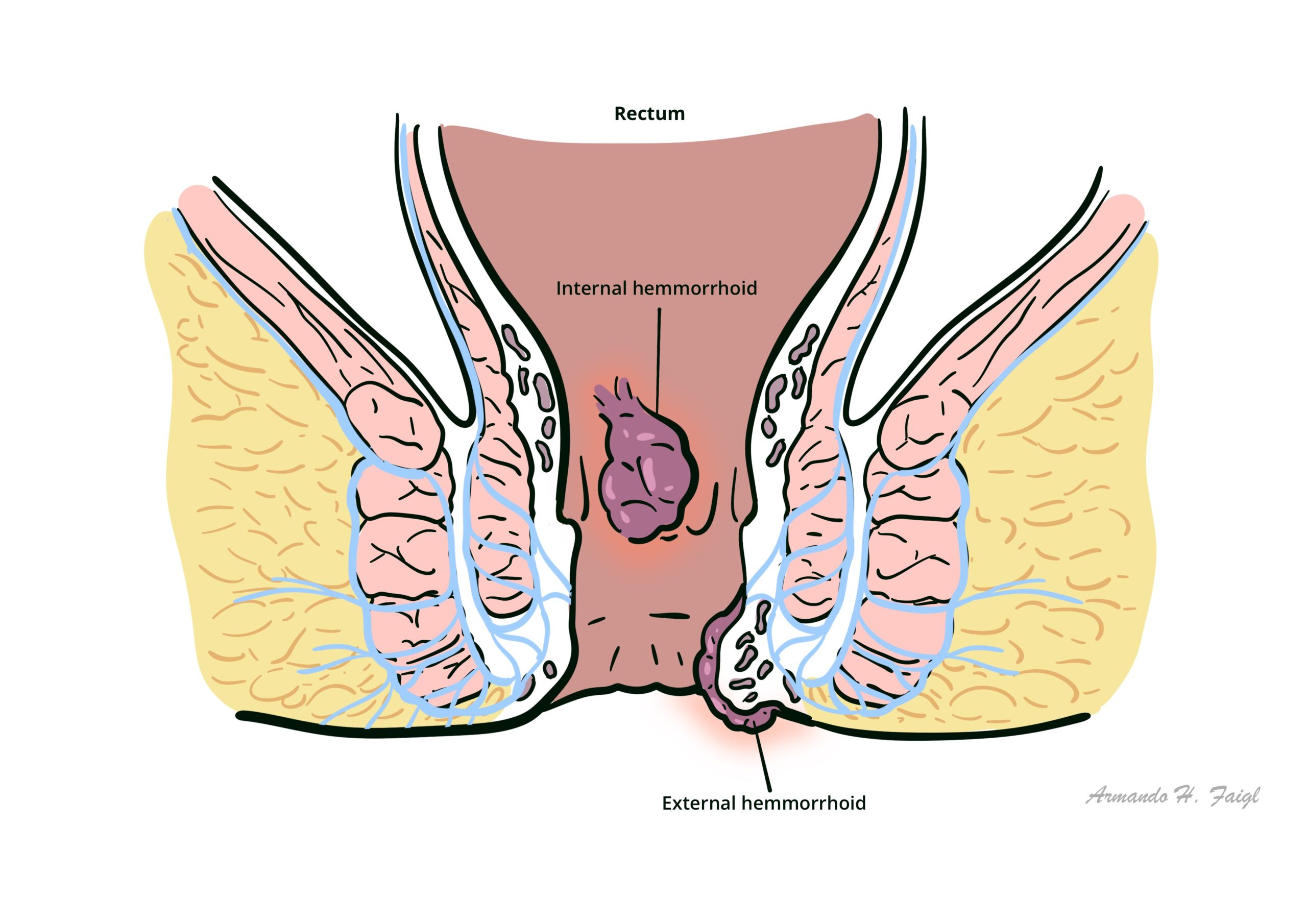
Haemorrhoid Plexi are normal anatomical structures located within the anal canal. The term “Anal Haemorrhoids” usually refers to a pathology where the Haemorrhoidal Plexi are enlarged. They are mainly caused by chronic constipation and frequent defecation leading to dilation and engorgement of haemorrhoidal tissue. Common symptoms are bleeding, pain and itching. There are internal and external haemorrhoids.
Definition
Haemorrhoid plexus: venous drainage of the anal canal being at the haemorrhoid plexi. There is an internal and external haemorrhoid plexus. Dilatation of a haemorrhoid plexus causes haemorrhoids.
Anal haemorrhoids: collections of submucosal, fibrovascular, arteriovenous sinusoids that are part of normal anorectum; sometimes referred to as “varicose veins” of the anorectum.
Internal haemorrhoids: originate proximal to the dentate line and are covered by insensate transitional epithelium.
Prolapsed haemorrhoids: severe and painful form of internal haemorrhoids that push through the anus and hang out of the body.
External haemorrhoids: located distal to the dentate line and are covered by sensate anoderm or skin.
Anatomy
Anal cushions – normal vascular cushions at 3, 7 and 11 o’clock positions; composed of venous sinusoids, connective tissue and smooth muscle. Their function is to help with anal continence by contributing to mucosal sealing; haemorrhoids as pathology occur when these cushions enlarge, prolapse and become symptomatic.
Typically haemorrhoids occur in the same location as the main anal blood vessels pedicles (described as 3, 7 and 11 o’clock positions as seen in the supine position).
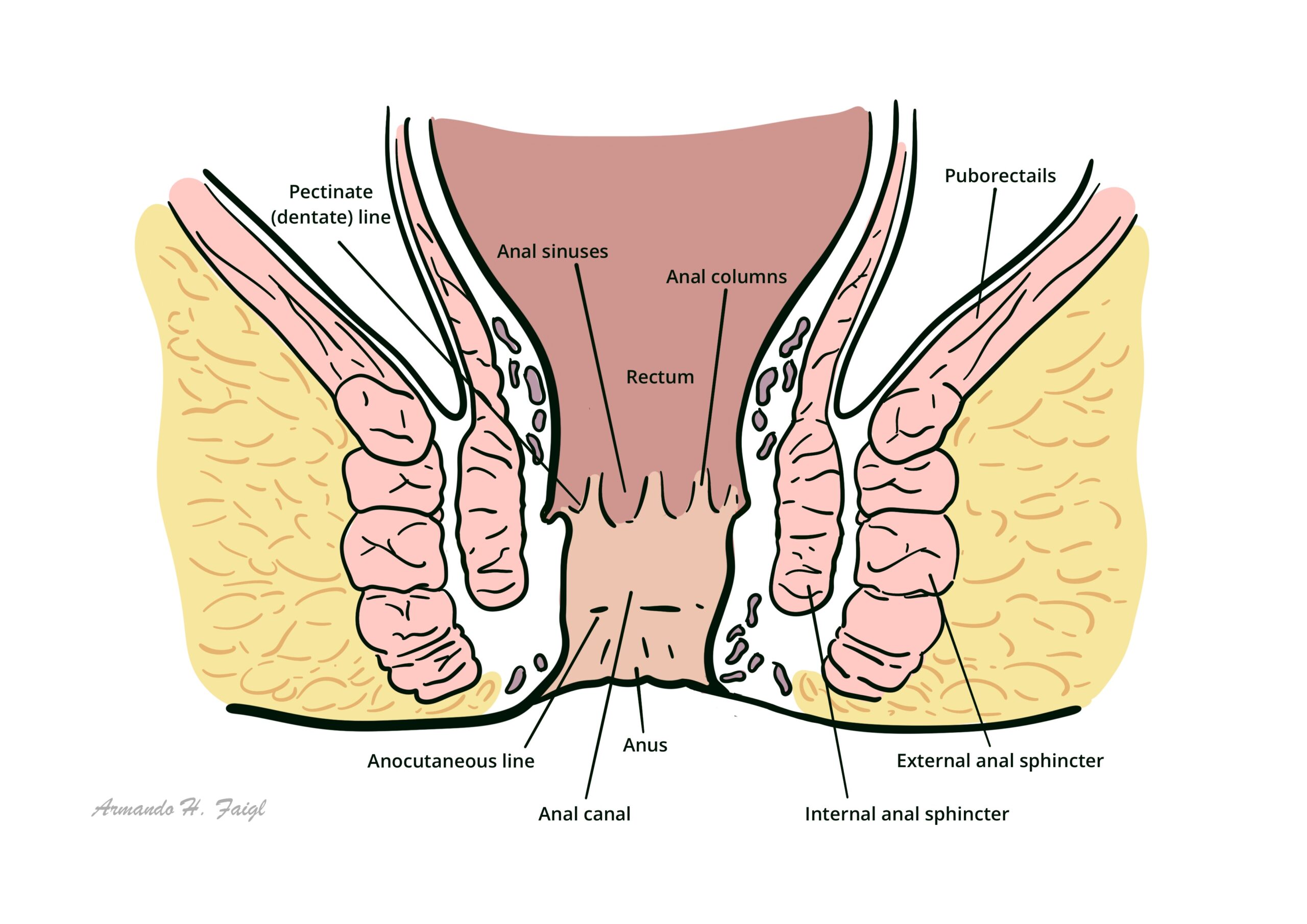
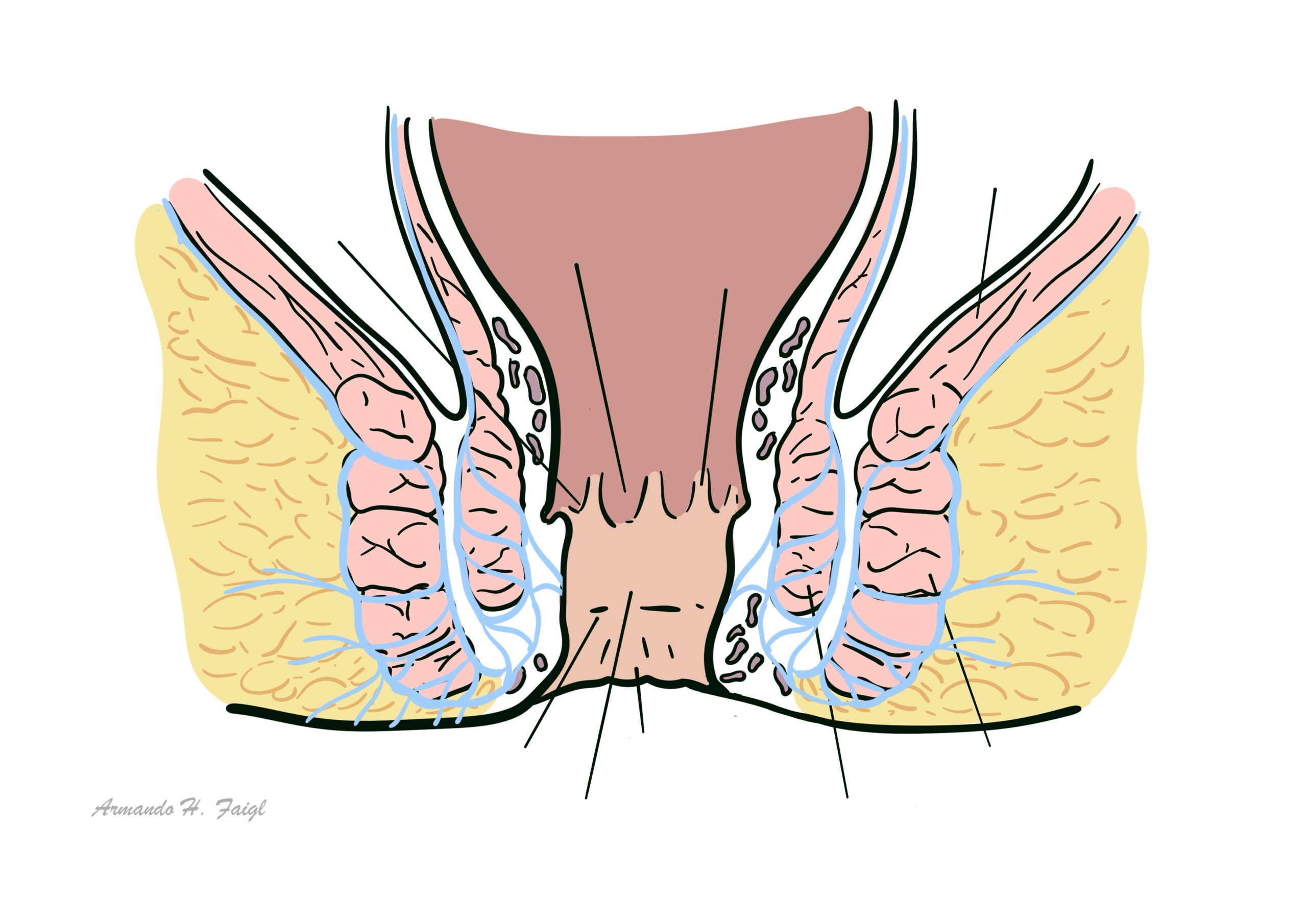
Anal canal – channel connecting the rectum to the anus, located within the anal triangle of the perineum, between the two ischioanal fossae.
Anal Sphincters
- Internal sphincter
- Involuntary control – continuation of circular fibers of the colon so it receives autonomic supply
- Surrounds upper 3/4 of anal canal
- External sphincter
- Voluntary control
- Surrounds entire length of anal canal
- Consists of three parts – subcutaneous, superficial and deep
Intersphincteric plane
- Between external sphincter muscle laterally and the longitudinal muscle (inner sphincteric muscle) medially
- Contains anal glands
- Can be opened up surgically to provide access for operations on the sphincter muscles
Anal glands
- Apocrine glands
- Occasionally infected and act as a source of anal fistula
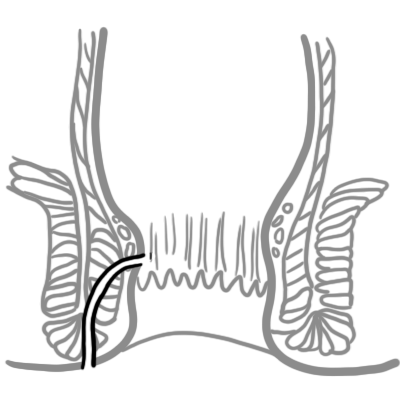
Dentate (pectinate) line
- Junction of the proximal and distal segments of the anal canal
- Divides the anus into proximal 2/3 and distal 1/3
- Situated at the middle of internal sphincter
| Distinction | Above Dentate line | Below Dentate line |
| Embryology | Hindgut (endoderm) | Proctodeum (ectoderm) |
| Epithelium | Columnar | Stratified squamous |
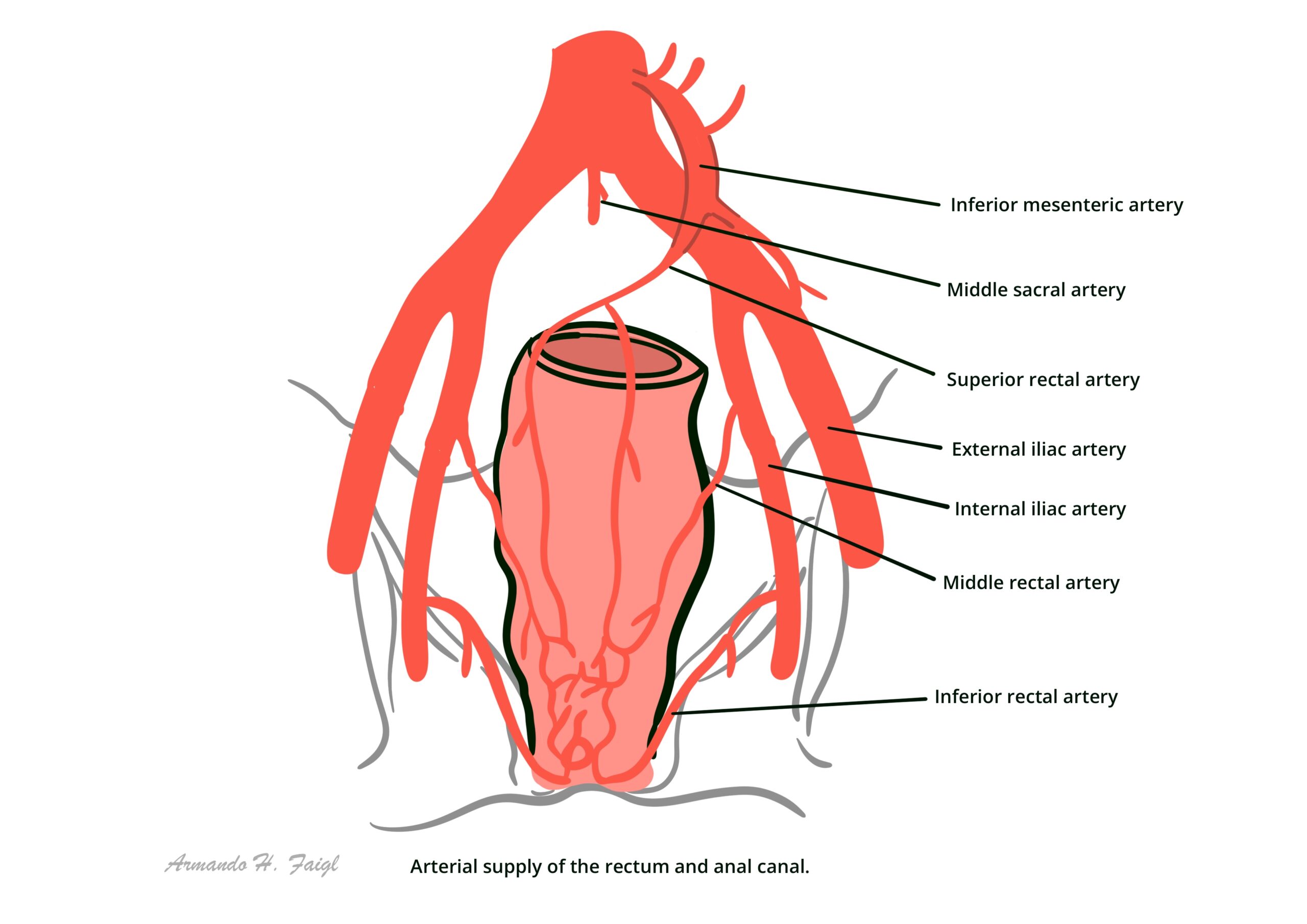
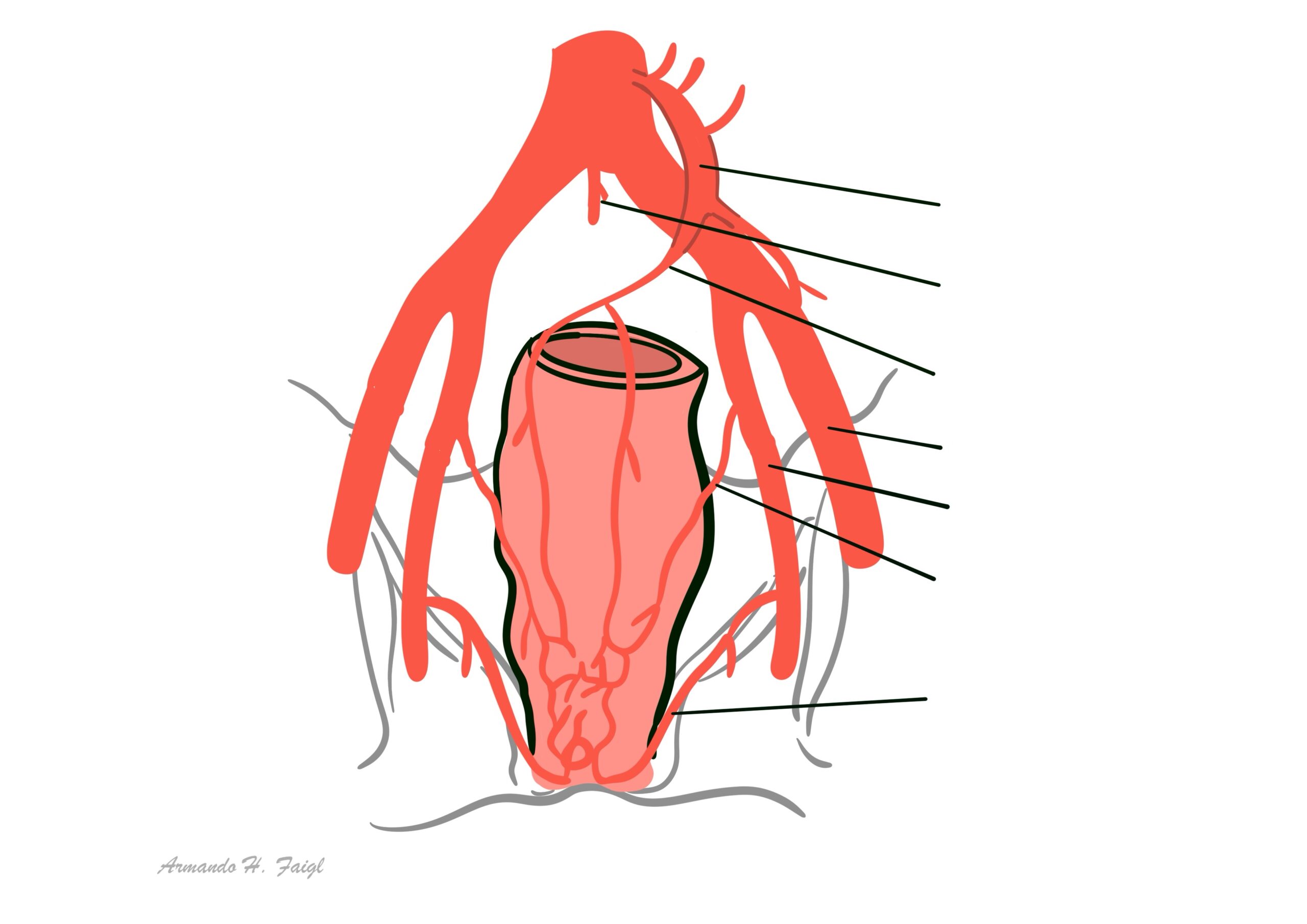
| Arterial supply | Superior rectal a. | Middle rectal a.Inferior rectal a. |
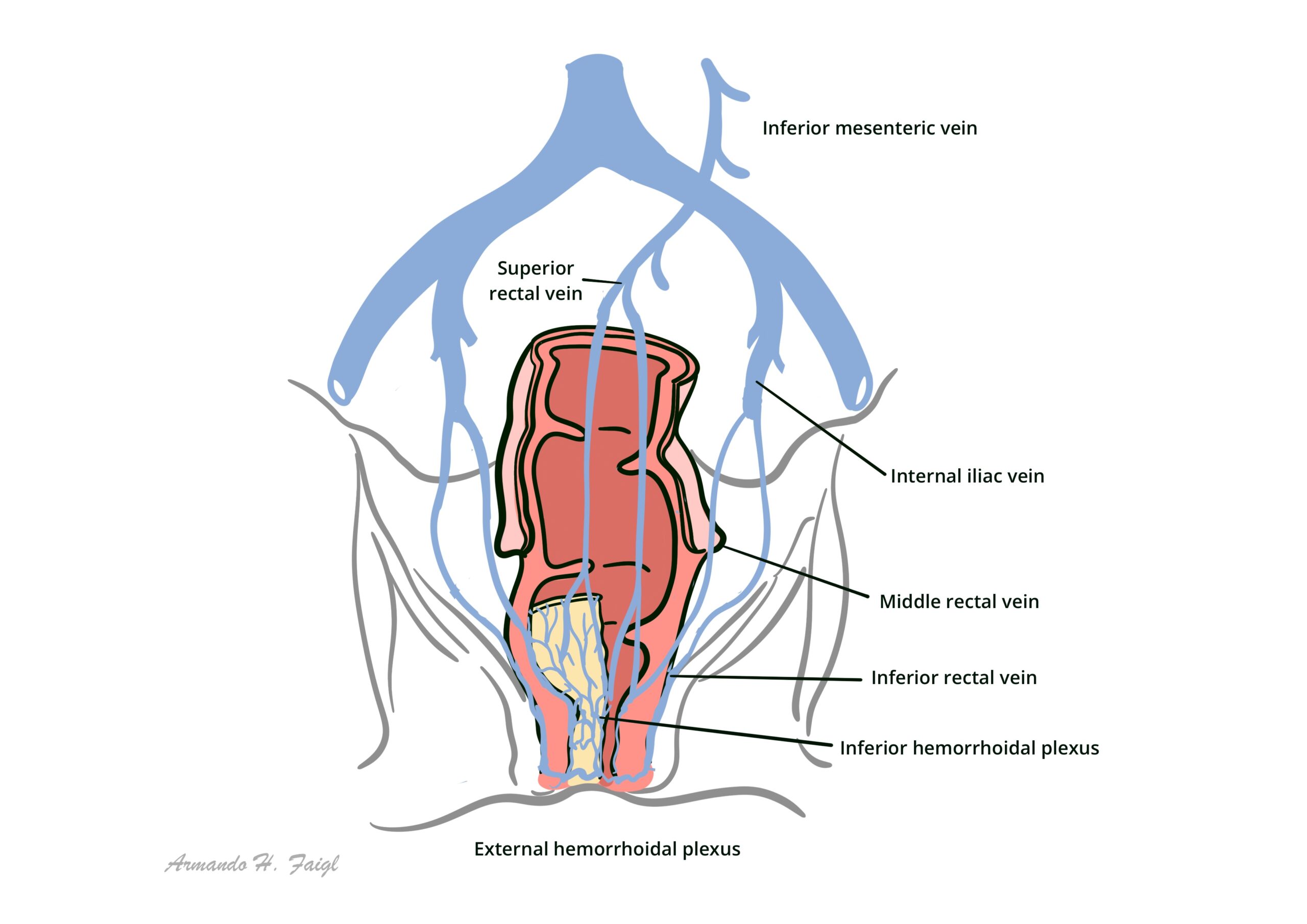
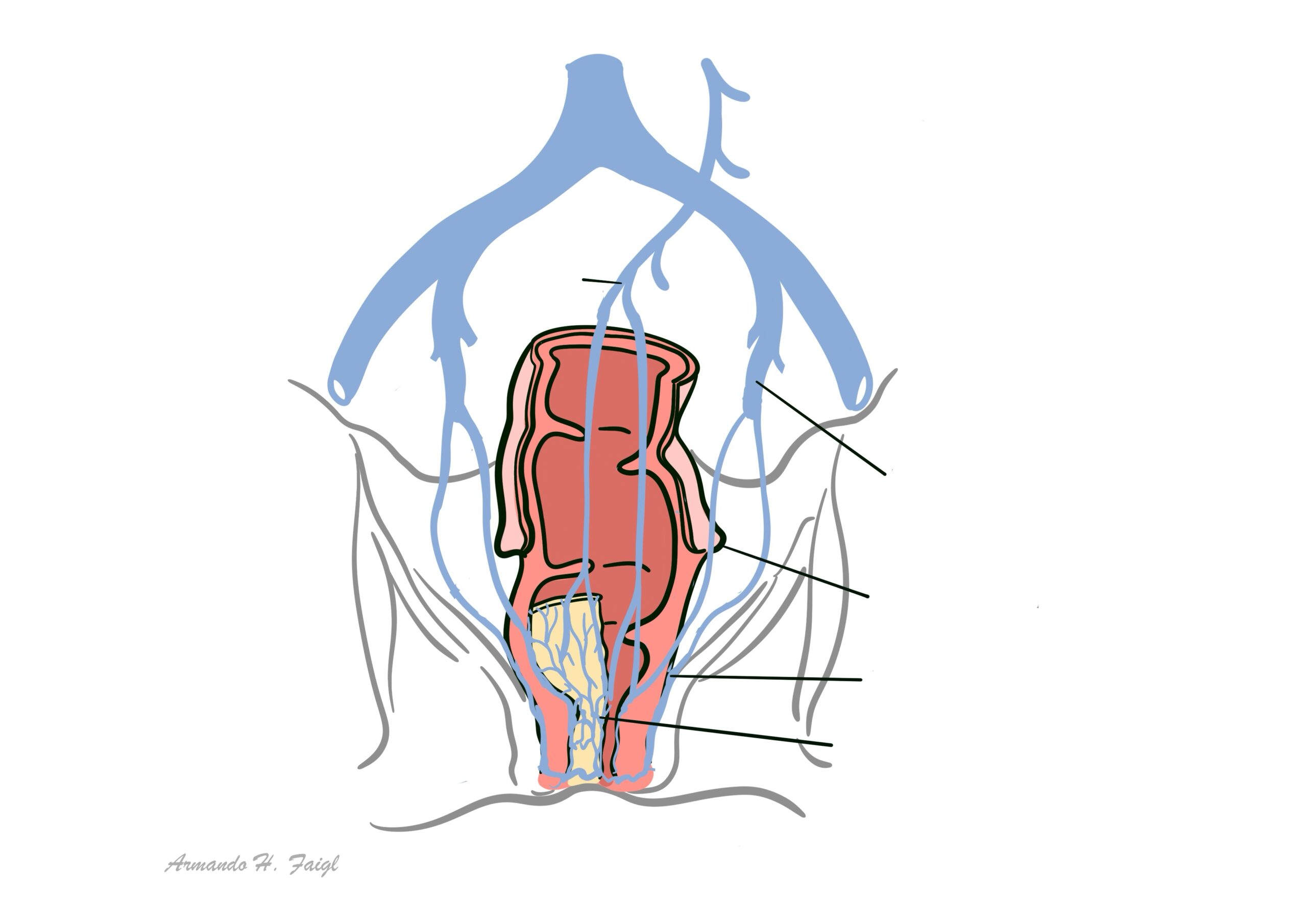
| Venous drainage | Superior rectal v. | Middle rectal v.Inferior rectal v. |
| Innervation | Visceral – Inferior hypogastric plexus(insensitive to pain) | Somatic – Inferior rectal nerves: branches of Pudendal nerve(sensitive to pain) |
| Lymph drainage | Internal iliac | Superficial inguinal |
| Haemorrhoids | Internal | External |
Hilton’s Line also called while line/anocutaneous line indicates lower end of the internal sphincter. Ischiorectal abscess when communicating with anal canal usually opens at or below Hilton’s line.
Aetiology & Risk factors
- Chronic constipation (most common)
- Low fiber diet
- Dehydration
- Medication side effects
- Chronic diarrhea
- Increased intraabdominal pressure
- Age (between 45 and 65)
- Spending long periods of time on toilet (eg. reading)
- Heavy lifting
- Chronic cough
Portal hypertension increases the risk of developing rectal varices, which present similarly to haemorrhoids.
Pathophysiology
Haemorrhoids are a normal component of the anal canal – they become pathological when they cause symptoms
↓
Increased venous pressure/weakening of supporting structures
↓
Engorgement of haemorrhoidal plexus/displacement of anal cushion
↓
Venous dilation and stasis
↓
Inflammation and oedema
↓
Clinical manifestations (bleeding, prolapse, pain, itching)
Classification
External haemorrhoids – below the dentate line; can form thrombus and cause severe pain that usually resolves after 2 weeks.
Internal haemorrhoids – above dentate line; can prolapse out of anal canal.
Clinical Manifestation
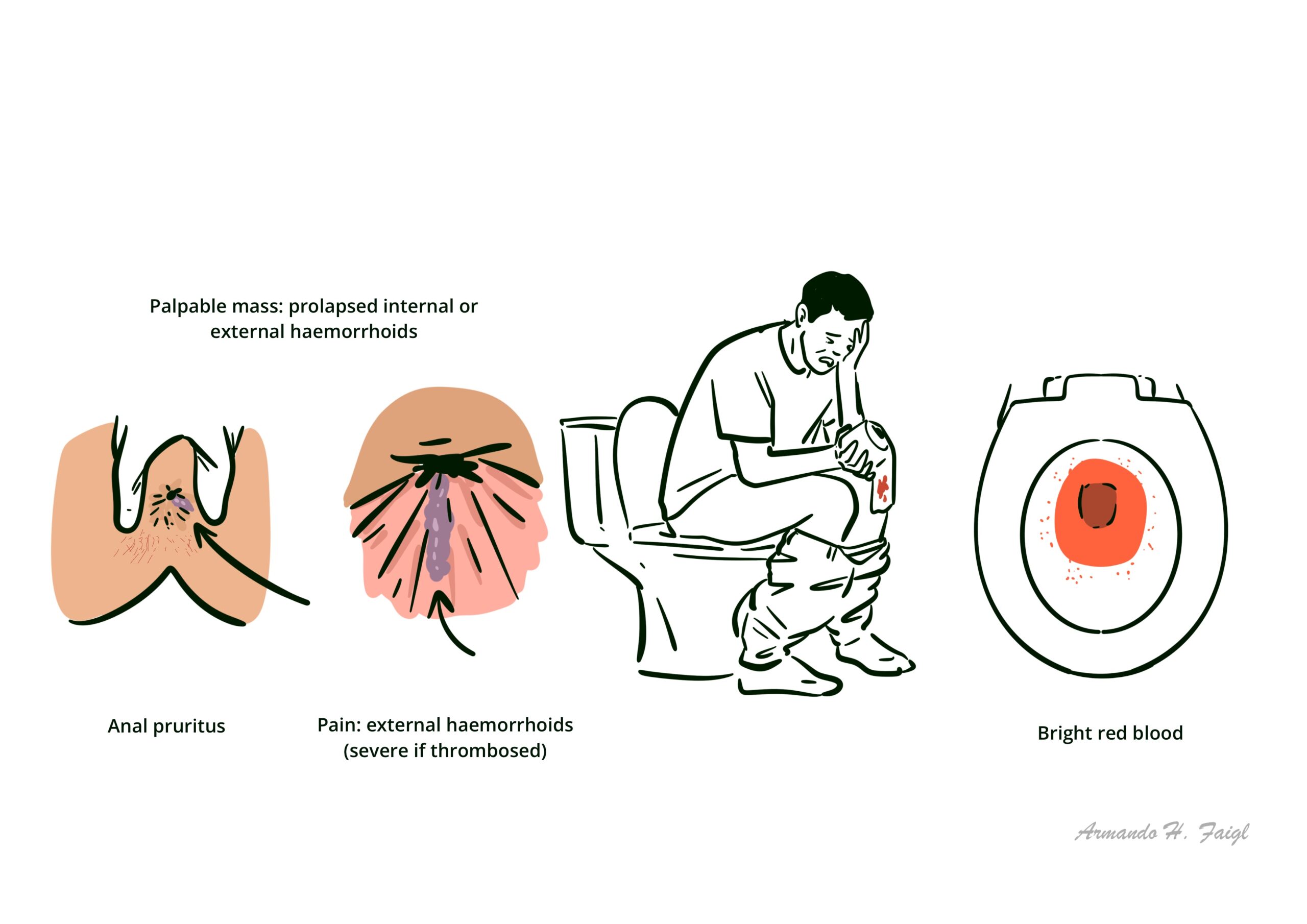
- Bleeding: bright red blood (on toilet paper, pain or coating stool – not mixed with it)
- Palpable mass: prolapsed internal or external haemorrhoids
- Pain: external haemorrhoids (severe if thrombosed)
- Anal pruritus: due to moisture associated with prolapsed internal haemorrhoid or difficulty to maintain hygiene 2,4

Although external thrombosed haemorrhoids causes severe pain, the presence of severe pain raises the possibility of other conditions, including anal fissure, perirectal or perivaginal infection, abscess, and other inflammatory processes.
Commonest age of onset is young adulthood.
Approximately 40% of haemorrhoids are asymptomatic.
Examination
- General inspection
- Visible haemorrhoids: either external or prolapsed internal
- Skin tags (resolved external hemorrhoids)
- Assess for thrombosis (tender, tense bluish lump)
- Prolapse on straining – ask patient to bear down
- Digital rectal exam (DRE): palpable internal lumps; evidence of bleeding
- Anoscopy – if history is suggestive of haemorrhoids but DRE inconclusive: bulging purplish-blue or dark pink masses, potentially tender
- Anal fissure
- Anal fistula
- Polyps
- Rectal prolapse
- Colorectal or anal cancer
- Rectal varices (due to portal hypertension)
- Proctitis
- Solitary rectal ulcer syndrome
Diagnosis
Anoscopy – most conclusive and specific tests for haemorrhoids
Endoscopic evaluation with colonoscopy or flexible sigmoidoscopy; indicated if:
- Patient is 40 years or older
- High suspicion of haemorrhoids but unable to detect on anoscopy
- Concerning clinical manifestations
- Iron deficiency anemia
- Risk factors for colonic disease
Labs – FBC (rarely performed): might show iron deficiency anaemia if significant bleeding (indicates endoscopic evaluation)
Treatment
General treatment (first-line)
- Increase dietary fibre and fluid intake
- Regular exercise
- Avoid straining while passing stool
- Avoid prolonged sitting on toilet
Medical treatment
- Sitz baths
- Stool softeners or bulk forming laxatives
- Steroid cream – temporary relief of some symptoms
- Pramoxine (anti-itching) – temporary relief of some symptoms
Surgical treatment
- Rubber band ligation – Stage I, II and III
- Infrared coagulation – Stage I and II
- Sclerotherapy – Stage I and II
- Stapled haemorrhoidopexy – Stage III
- Haemorrhoidal artery ligation – Stage III
- Surgical haemorrhoidectomy – Stage IV and mixed (combined external and internal haemorrhoids)
Avoid constipation/straining. Exercise, high-fiber diet and drinking plenty of water are good recommendations.
Complications & Prognosis
- Anaemia
- Pain
- Heavy bleeding
- Chronic unremitting prolapse of mucosal tissue
- Strangulation
- Ulceration
- Thrombosis
- External haemorrhoids are usually self-limiting and patients live with existing lumps
- Rubber banding is a good treatment with good outcome
References
1. Community HealthPathways. Haemorrhoids: Hunter New England; [cited 2025 Sep 20]. Available from: https://hne.communityhealthpathways.org/13803.htm.
2. BMJ Best Practice. Haemorrhoids [updated 27 September 2024; [cited 2025 Sep 20]. Available from: https://bestpractice.bmj.com/topics/en-gb/181.
3. American Society of Colon & Rectal Surgeons. Hemorrhoids [cited 2025 Sep 20]. https://fascrs.org/patients/diseases-and-conditions/a-z/hemorrhoids
4. healthdirect. Haemorrhoids [cited 2025 Sep 20]. Available from: https://www.healthdirect.gov.au/haemorrhoids-piles.
5. GP Exams. Haemorrhoids [cited 2025 Sep 20]. Available from: https://gpexams.com/haemorrhoids/.
6. Bleday R, Breen E. Hemorrhoids: Clinical manifestations and diagnosis [updated 2025 Sep 11; cited 2025 Sep 20]. Available from: https://www-uptodate-com.ezproxy.newcastle.edu.au/contents/hemorrhoids-clinical-manifestations-and-diagnosis.









Members only discussions coming soon…