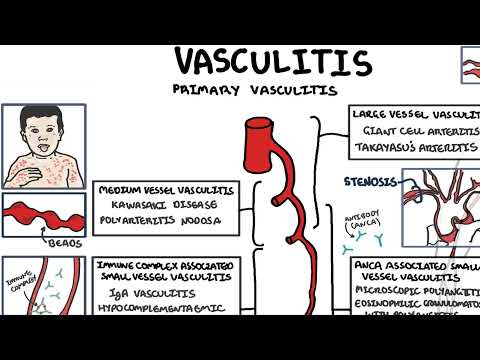
0:00 Hello, in this video we're going to talk about large vessel vasculitis, this is 0:12 an overview. 0:14 Vasculitis is inflammation of the blood vessels, resulting in damaged vessels, 0:18 leading to potential 0:20 complications such as tissue ischemia and also aneurysms. 0:27 Very vascularities are classified into the size of the blood vessels affected. 0:32 Large vessel, medium vessel and small vessel vasculitis. 0:38 In this video we're going to focus on large vessel vasculitis, which typically 0:42 affects 0:42 the aorta and its main branches. 0:45 The large vessel vasculitis include giant cell arthritis and tachyatsu 0:53 arthritis. 0:55 Cell arthritis, GCA, also known as temporal arthritis, is defined as granulomat 1:01 ous arthritis 1:02 of the aorta and the large vessels. 1:05 It typically affects the aorta and/or its major branches. 1:11 Here is the left common carotid artery branch of the aorta. 1:15 The common carotid then divides into the internal and external carotid arteries 1:20 . 1:21 The external carotid artery has many branches, including the superficial 1:28 temporal artery. 1:29 Usually, giant cell arthritis presents in the elderly population with a higher 1:34 propensity 1:35 towards females. 1:38 A new nonspecific, usually severe headache neck pain, tenderness along the 1:45 temporal artery 1:46 and visual changes should raise suspicion of a giant cell arthritis. 1:53 Looking at the artery affected, the histopathological findings include presence 2:00 of giant cells. 2:01 There is pan-artritis, inflammation of all the vessel layers. 2:07 Presence of CD4 and CD8 lymphocytes and macrophages. 2:13 All these cells are usually found in the smoother muscle layers of the vessel 2:18 in giant cell 2:19 arthritis. 2:22 A characteristic of giant cell arthritis is that the inflammation of the blood 2:26 vessel 2:27 occurs in segments along the artery, like skip lesions. 2:32 When there is any potential injury to the blood vessel, especially to the endot 2:36 helial 2:37 layer, hemostasis occurs, which include thrombosis and fibrin mesh. 2:45 However, in giant cell arthritis, on histopathology, there is no evidence of 2:52 fibrinoid necrosis, 2:54 and this is because fibrinoid necrosis is a histopathological term limited to 2:58 small blood 2:59 vessels. 3:00 These T lymphocytes and macrophages and giant cells, I mentioned, contribute to 3:05 the inflammatory 3:06 process seen in giant cell arthritis. 3:09 Important to know that giant cells are not a requisite for the diagnosis. 3:17 As mentioned, the classic presentation is an elderly lady with a new headache, 3:21 neck pain, 3:22 with usually a tender, potentially superficial temporal artery, which is 3:27 affected. 3:28 Visual changes are common and include transient visual loss, called amorosis 3:34 fugex, or even 3:36 complete visual loss. 3:38 If the facial artery is affected, jaw clodication can occur. 3:43 If the lingual artery is affected, tongue clodication can occur. 3:47 Symptoms of jaw and tongue clodication, such as pain when eating and chewing, 3:51 is highly 3:52 specific for giant cell arthritis. 3:56 Polymyelgeorimatica is also closely linked to giant cell arthritis, occurring 4:00 in up to 4:01 50% of patients who have giant cell arthritis. 4:08 Investigations for suspected giant cell arthritis, or vasculitis, include blood 4:12 s, looking for 4:13 ESR, the erythrocyte sedimentation rate, which is a long-term inflammatory 4:19 marker, 4:20 and then there's also the CRP, which is C-reactive protein, a short-term 4:24 inflammatory marker. 4:27 An ultrasound doppler of the superficial temporal artery can also be made, 4:32 which may have signs 4:33 of archery stenosis, or a halo sign. 4:37 Here is an example of an ultrasound doppler of the temporal artery, showing the 4:45 halo sign. 4:46 Diagnosis of giant cell arthritis is made through a temporal artery biopsy, and 4:50 the biopsy 4:51 should typically be a good chunk of the artery, because remember, the hallmark 4:56 of giant cell 4:57 arthritis are the skip lesions. 5:01 Also in the biopsy, the other finding I mentioned earlier includes immune cell 5:05 infiltration in 5:06 a smooth muscle layer, and also evidence of pain arthritis. 5:13 Diagnosis should not delay treatment because of the risk of organ ischemia, 5:16 including 5:17 visual loss and dual predication. 5:21 Giant cell arthritis requires high dose of glucocorticoids, which will be tape 5:26 red slowly 5:27 over 6-12 months. 5:29 Important to keep in mind the risk of osteoporosis, especially in the elderly 5:33 female population 5:34 group. 5:36 Calcium and vitamin D supplements and oral or IV bisphosphonates are essential. 5:43 The next large vessel vasculitis is takayatsu artritis. 5:50 Takayatsu artritis is also known as postless disease, and it is a granulomatus 5:55 artritis 5:55 that predominantly affects the aorta and the great vessels. 6:01 It is named after the Japanese professor Mikito Takayatsu, who first described 6:05 the findings 6:06 of the disease in a young population Japanese group. 6:10 Unlike giant cell arthritis, which typically affects elderly women, takayatsu 6:15 artritis 6:16 is more common in young women and is highly prevalent in the Asian population. 6:23 The pathological change that occur in takayatsu artritis is similar to giant 6:27 cell arthritis. 6:29 The large arteries such as the aorta is affected. 6:32 On histopathology there is panartritis, and even you can see giant cells. 6:39 In takayatsu however, lumen narrowing of the aortic arch and branches are 6:43 common. 6:44 The lumen narrowing is due to a number of mechanisms. 6:47 Firstly, infiltration of cells leading to inflammation and destruction to the 6:52 vessel 6:52 layers. 6:53 Secondly, thrombosis and fibrin mesh as a mechanism of repair. 6:58 Thirdly, hyperplasia fibrosis and thickening of the arterial wall as a result 7:04 of the inflammation. 7:06 The other important feature of takayatsu is that it is arthritis of the aorta 7:11 and the 7:12 great vessel. 7:14 Pulmonary arteries and abdominal arteries occur in 50% of cases. 7:20 The clinical feature of takayatsu, as we mentioned earlier, is that usually the 7:25 population group 7:26 are females and younger than 40. 7:31 The main branches of the aortic arch supplies blood to the head, neck, and 7:35 upper limbs. 7:36 If there is damage to these large vessels, patients can present with decreased 7:39 pulse 7:40 strength or even absent pulse. 7:43 Hordication of the extremities if the narrowing of the artery is so great. 7:49 Hypertension can also occur and this is due to decreased blood flow to the 7:53 kidneys. 7:53 When there is decreased blood flow to the kidneys, the kidneys will release ren 7:57 in which 7:57 will subsequently activate the renin and your tins and aortosterone system to 8:02 increase the 8:03 blood pressure. 8:05 Because the right subclavian artery and left subclavian artery can be affected 8:10 to varying 8:11 degrees, there can be a difference at discrepancy in blood pressure between 8:16 each arm, typically 8:18 a difference of at least 10 millimeters mercury. 8:22 Decreased blood supply to the head leads to lightheadedness and headaches. 8:27 An interesting phenomenon called subclavian steel syndrome can also occur where 8:32 due to 8:32 reduced blood flow through the left subclavian, the left subclavian will 8:39 essentially steal 8:40 blood from the carotid artery through the circle of willis in the brain. 8:46 Finally, arterial bruise in the abdomen may be heard. 8:50 Biopsy of the large vessels is impractical and not really done. 8:57 Researchers of Takayatsu arthritis is often incidentally found when a CT chest 9:04 is performed. 9:05 Diagnosis rests largely on clinical findings with the help of imaging, angi 9:10 ography such 9:11 as an MRI angiogram which shows areas of stenosis along the aorta and its 9:18 branches. 9:19 And also laboratory studies such as raised ESI and CRP can help support the 9:25 diagnosis. 9:26 Leukocorticoids are first line treatment, however in patients with steroid 9:31 resistant 9:32 disease, alternatives such as meth or trexate, as a thiopurine and mycofenolate 9:39 may be given. 9:41 Angioplasty can also help in symptomatic relief where an endovascular wire with 9:46 a balloon 9:47 is used to help widen the artery to improve blood flow and circulation. 9:56 [BLANK_AUDIO]