Goodpasture Syndrome (Anti-GBM disease)

Goodpasture syndrome, now more precisely termed anti-glomerular basement membrane (anti-GBM) disease, is a rare autoimmune small-vessel vasculitis affecting lungs and kidneys, typically manifesting with diffuse alveolar hemorrhage and rapidly progressive glomerulonephritis.
Microscopic polyangiitis (MPA) has an estimated incidence of approximately 0.5 to 1.8 cases per million per year. It demonstrates a bimodal age distribution, with peaks occurring between 20–30 years and again between 60–70 years. There is a male predominance. Genetic associations include HLA-DR15 and HLA-DR4, and environmental triggers such as smoking and hydrocarbon exposure have also been implicated in disease development.
Anti-GBM disease: autoimmune condition where antibodies target the α3-NC1 domain of type IV collagen in glomerular and alveolar basement membranes
Pulmonary-renal syndrome: simultaneous involvement of lungs (hemorrhage) and kidneys (glomerulonephritis).
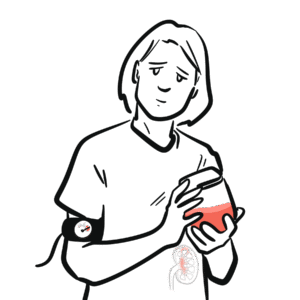
Rapidly progressive glomerulonephritis (RPGN): rapid loss of kidney function often with crescents on biopsy, can be manifestation of anti-GBM disease.
Type II hypersensitivity: immune reaction where antibodies bind antigens on tissues, causing complement fixation and inflammation (mechanism here).
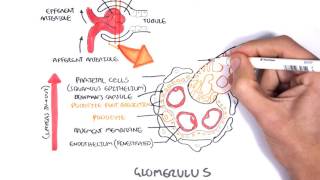
Relevant normal anatomy/physiology without disease:
Aetiology: Autoantibodies directed against the non-collagenous (NC-1) domain of α3 chain of type IV collagen in lung and kidney basement membranes
genetic predisposition creates susceptibility—but environmental “hits” often precipitate disease.
early damage to barrier exposes hidden antigens, tipping into autoimmune cascade.
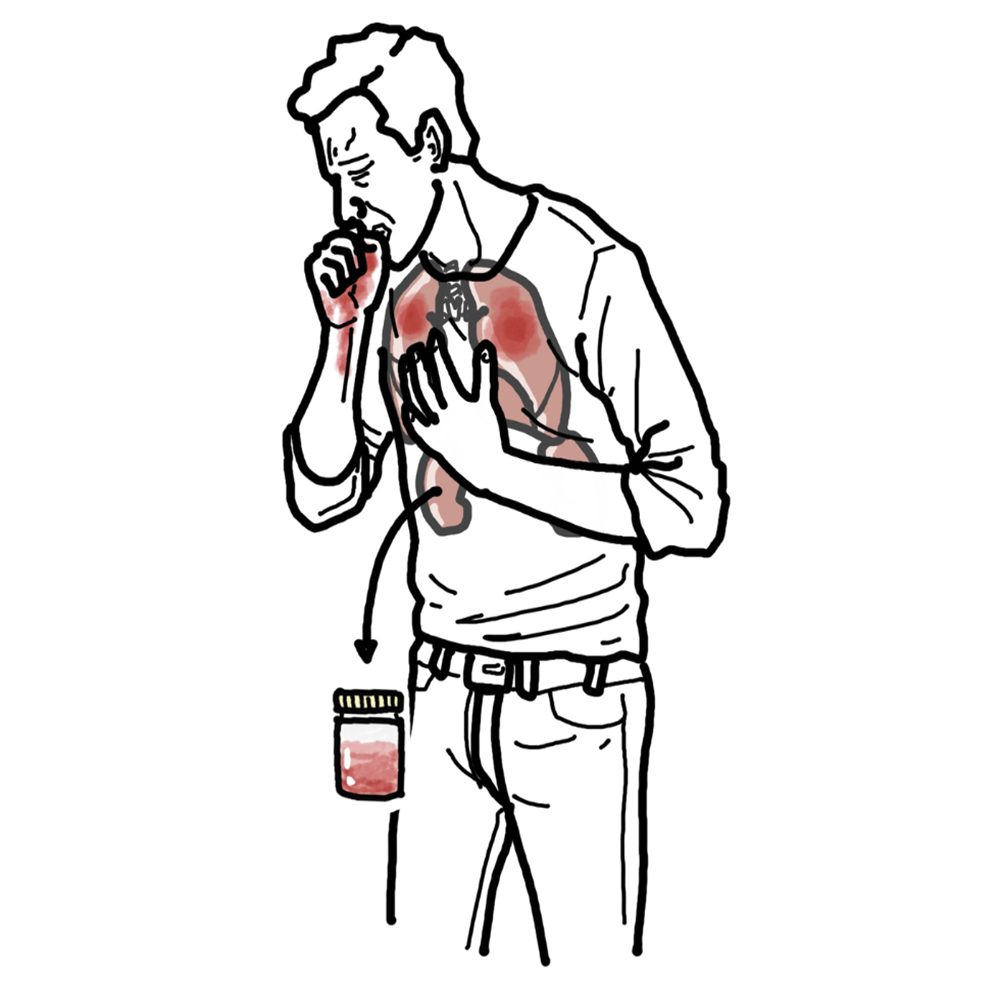
Triad: hemoptysis + glomerulonephritis + anti-GBM antibodies — diagnostic triad of Goodpasture syndrome.
absence of hemoptysis does NOT rule out pulmonary involvement.
Differential diagnoses
Supportive care: dialysis for renal failure; respiratory support or intubation for pulmonary hemorrhage
Complications
• Renal failure requiring long-term dialysis or transplant.
• Recurrent pulmonary hemorrhage.
• Infections due to immunosuppression.
• Rare relapse.
Prognosis:
• With early treatment: 5-year survival ~80%, >80% overall initial survival [8,4].
• Without treatment: nearly universally fatal.
• Poor prognostic factors: dialysis dependence at presentation, high creatinine, extensive crescents, delayed treatment
early intervention markedly improves outcomes.















Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion