

Reactive Arthritis
Overview
Reactive arthritis is a seronegative spondyloarthropathy that occurs after a genitourinary or gastrointestinal infection, typically presenting as an asymmetric oligoarthritis, often with associated conjunctivitis and urethritis (formerly Reiter’s syndrome). It most commonly affects young adults aged 20–40 and shows a strong association with HLA-B27. Incidence is estimated at 30–40 per 100,000, with higher rates in HLA-B27–positive individuals following infection.
Definition
Reactive arthritis: Sterile inflammatory arthritis occurring 1–6 weeks after infection.
Seronegative spondyloarthropathy: Group of inflammatory arthritides negative for RF/anti-CCP.
Enthesitis: Inflammation at sites of tendon/ligament insertion.
Dactylitis: Diffuse swelling of an entire digit due to synovitis and tenosynovitis.
Anatomy and Physiology
Aetiology and Risk Factors
- Infectious triggers (precede arthritis by ~1–4 weeks):
- GU: Chlamydia trachomatis
- GI: Salmonella, Shigella, Yersinia, Campylobacter, Clostridium difficile
- HLA-B27 positivity (increases risk and severity)
- Young age (20–40 years)
- Male sex (especially with genitourinary infections)
- Immunogenetic susceptibility
Always ask about recent diarrhoea, dysuria, or STI symptoms in young patients with new arthritis.
Pathophysiology
- Initial GI or GU infection triggers immune activation
- Bacterial antigens persist in synovium or gut mucosa (molecular mimicry)
- Dysregulated immune response involving CD8+ T cells, cytokines (IL-17, TNF-α)
- Results in sterile synovitis, enthesitis, and extra-articular inflammation
Arthritis in ReA is sterile — no live organisms are found in the joint.
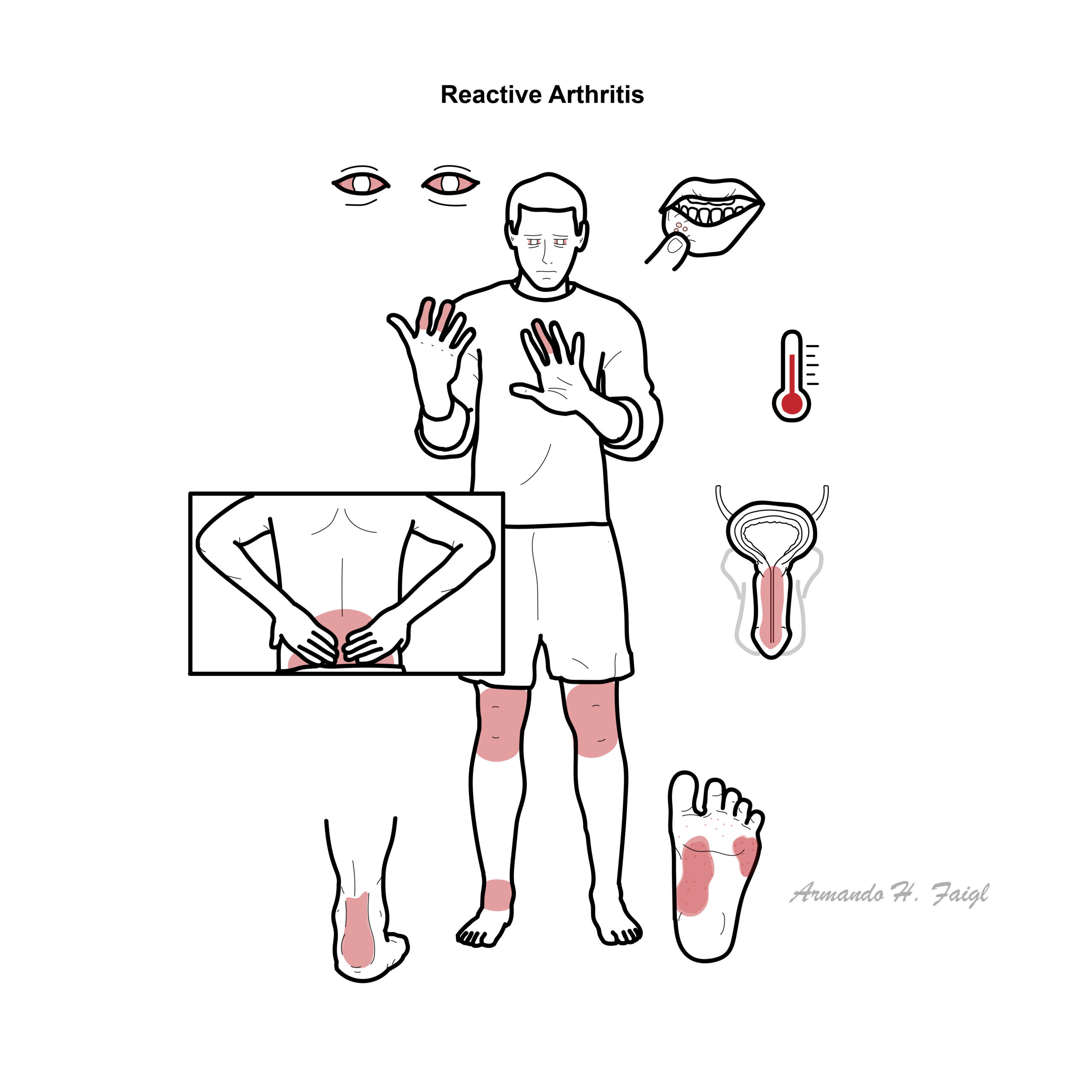
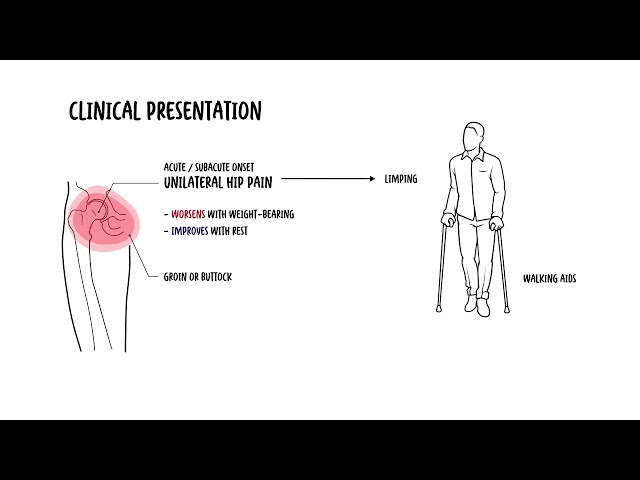
Clinical Manifestations
- Arthritis
- Asymmetric oligoarthritis (knees, ankles, MTPs)
- Dactylitis (“sausage digit”)
- Heel pain (enthesitis)
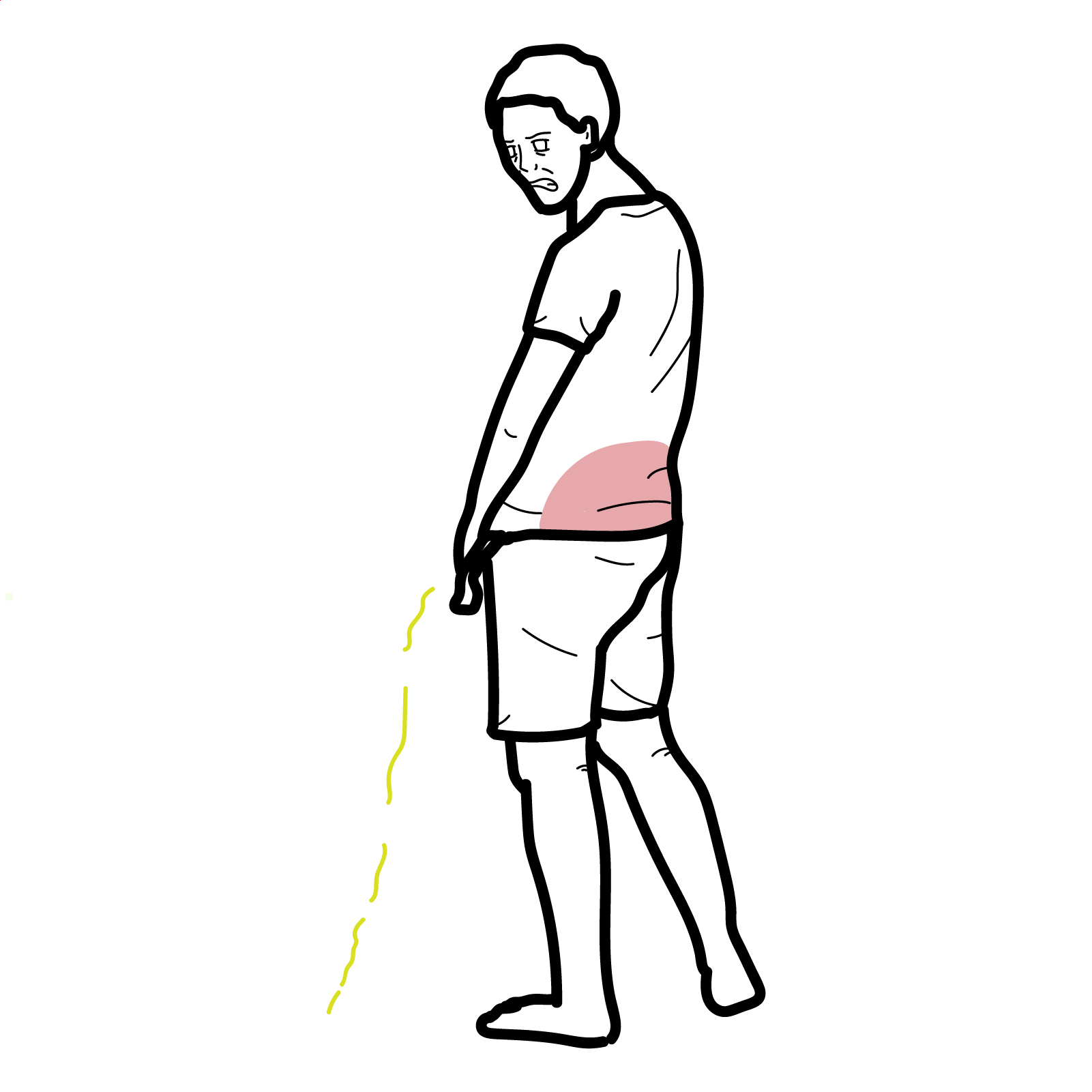
- Lower back pain (sacroilitis)
- Ocular Conjunctivitis (mild), anterior uveitis (painful)
- Urogenital: Urethritis, cervicitis, prostatitis
- Mucocutaneous:
- Oral ulcers
- Circinate balanitis
- Keratoderma blennorrhagicum (psoriasiform rash)
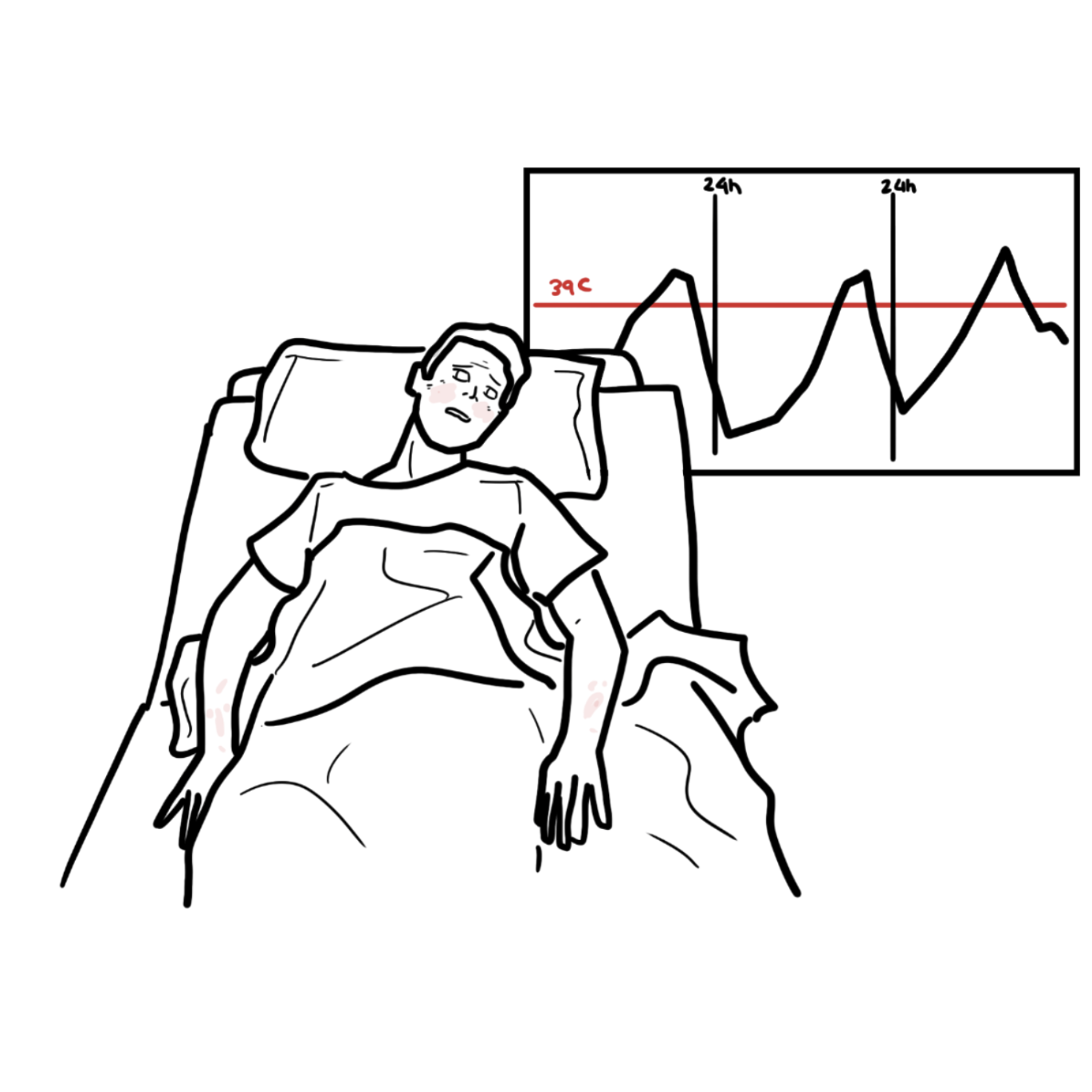
- Systemic symptoms: Fever, malaise, weight loss
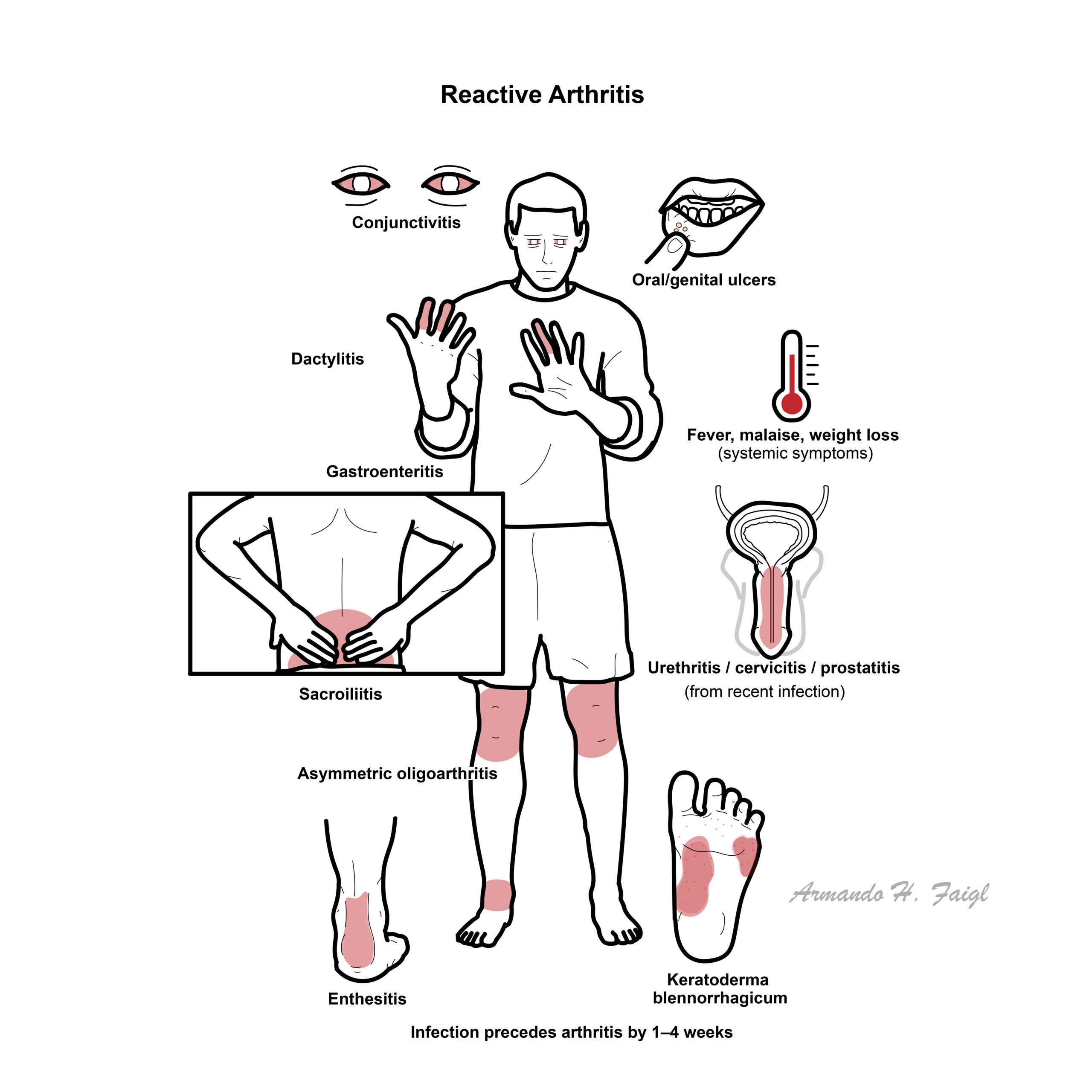
Triad: Arthritis, conjunctivitis, urethritis (Reiter’s syndrome — classic but rare today).
Diagnosis
No dedicated ReA classification criteria. Often diagnosed clinically based on:
– Acute oligoarthritis
– Preceding GI/GU infection
– Absence of live pathogen in joint fluid
- Stool or urine PCR/culture: to identify trigger organism
- HLA-B27 testing: positive in ~50–80% of cases
- CRP/ESR: often elevated
- Joint aspiration: to rule out septic arthritis (crystals, WBCs, culture)
- X-ray/MRI: May show periostitis, enthesitis, sacroiliitis in chronic cases
Differential Diagnoses:
| Condition | Differentiating Features |
| Septic arthritis | Fever, single joint, positive culture |
| Gonococcal arthritis | Young sexually active adults, migratory arthritis, tenosynovitis, skin pustules. Positive culture. |
| Viral Arthralgia | Joint pain without swelling following viral illness |
| Gout | Crystals in joint aspirate, often 1st MTP |
| Psoriatic arthritis | Skin/nail psoriasis, symmetric or axial involvement |
| IBD-related arthritis | History of Crohn’s/UC, gut symptoms |
Negative joint cultures + history of recent infection = key to diagnosis.
Treatment
- NSAIDs: first-line for arthritis and enthesitis
- Intra-articular corticosteroids: for persistent monoarthritis
- Short course oral corticosteroids: if polyarthritis or systemic symptoms
- Antibiotics: only if infection is still active (e.g. Chlamydia)
Chronic/refractory disease
- DMARDs: sulfasalazine or methotrexate for persistent arthritis
- Anti-TNF agents: for chronic or axial disease unresponsive to DMARDs
Supportive: Physiotherapy, sexual health counselling, patient education
Treat the infection first if active; otherwise focus on joint symptoms.
Complications and Prognosis
- Most cases resolve within 3–6 months
- ~30% may have chronic arthritis or relapsing flares
- Chronic ReA more likely with HLA-B27, severe initial disease, or poor treatment response
- Extra-articular complications (e.g. uveitis, enthesitis, sacroiliitis) may persist
- Rare: aortic valve involvement, amyloidosis
Poor Prognostic Factors
- HLA-B27 positivity
- Chronic sacroiliitis
- High inflammatory markers
- Recurrent infection
References
- Hannu T. Reactive arthritis. Best Pract Res Clin Rheumatol. 2011;25(3):347–357.
- Colmegna I, Cuchacovich R, Espinoza LR. HLA-B27-associated reactive arthritis: pathogenetic and clinical considerations. Clin Microbiol Rev. 2004;17(2):348–369.
- Braun J, Kingsley G, van der Heijde D, Sieper J. On the difficulties of establishing a consensus definition of reactive arthritis. J Rheumatol. 2000;27(10):2185–2187.
- Carter JD, Hudson AP. Reactive arthritis: clinical aspects and medical management. Rheum Dis Clin North Am. 2009;35(1):21–44.







Members only discussions coming soon…