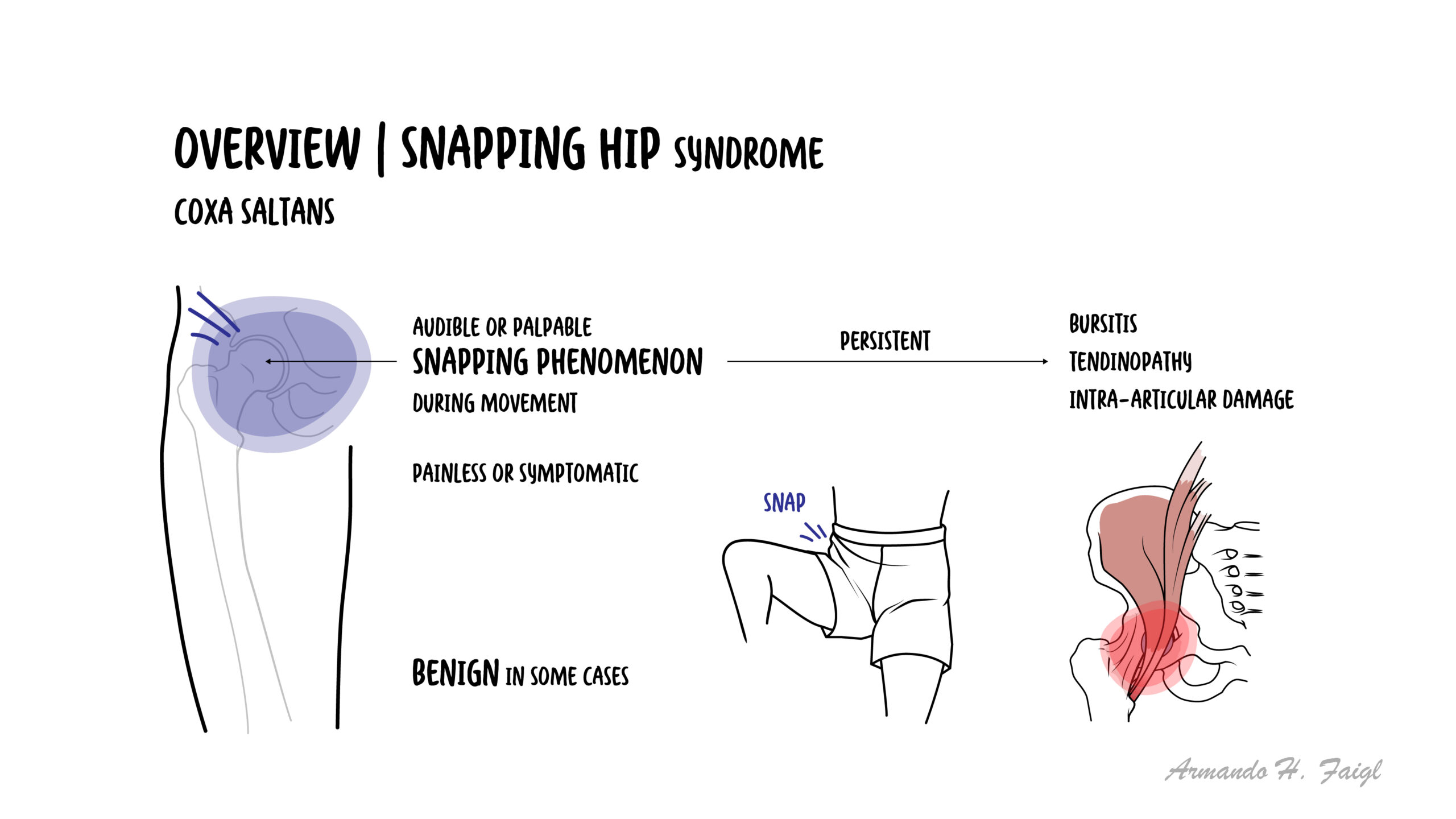
Snapping Hip Syndrome (SHS) is characterized by an audible or palpable “snap” around the hip during motion; it may be painless or painful and can be unilateral or bilateral. Prevalence estimates suggest up to ~5–10% of the general population may experience snapping to some degree, with higher rates in dancers and athletes who work their hips through extreme ranges of motion. Most cases respond to conservative care.
Definition
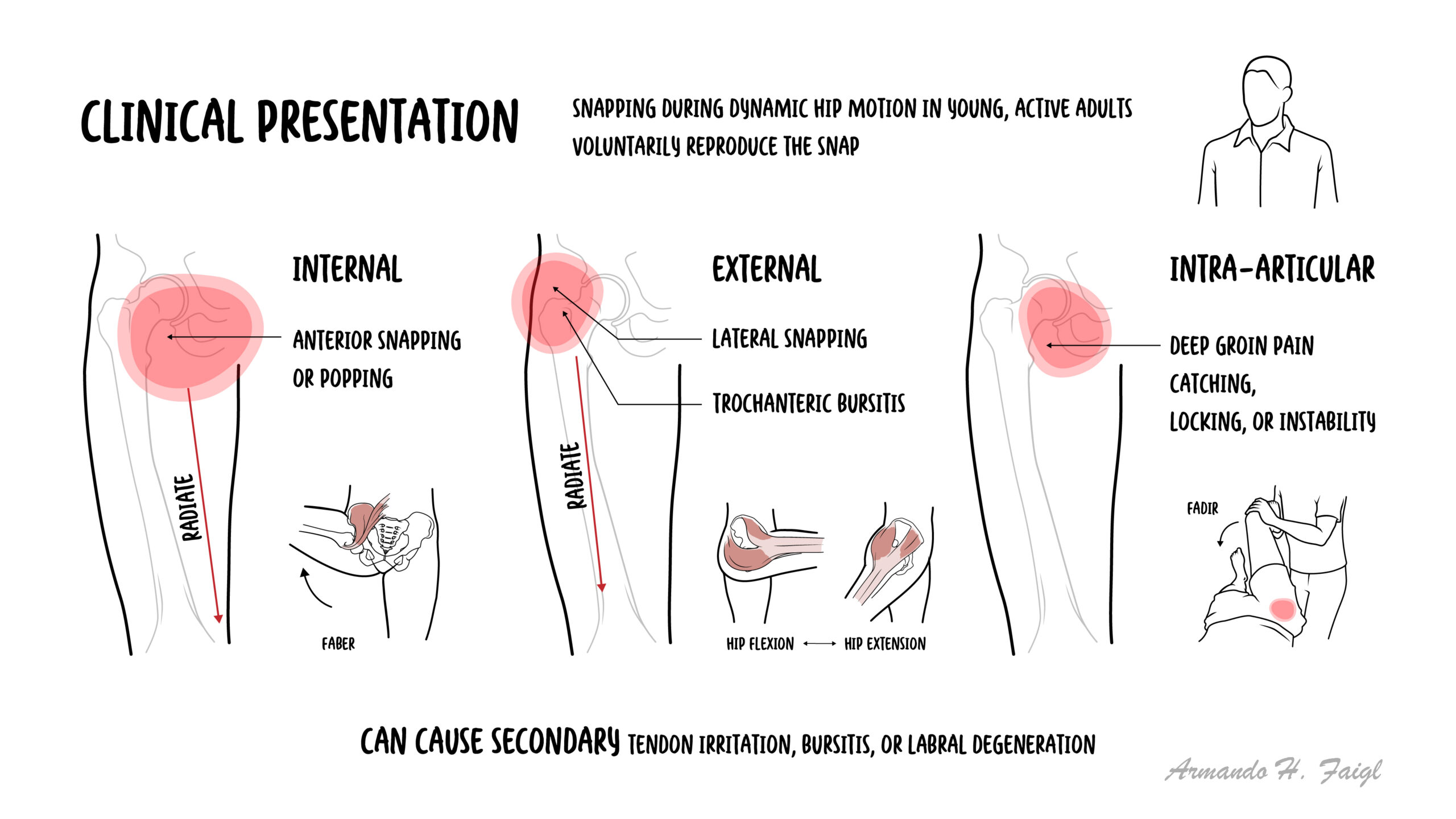
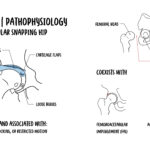
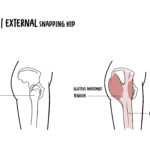
Coxa saltans: Latin for “snapping hip”; reproducible audible/palpable snap with hip motion, painful or painless. Internal snapping: Iliopsoas tendon translocates over bony/ capsuloligamentous prominences anteriorly (e.g., iliopectineal eminence). External snapping: ITB or anterior fibers of gluteus maximus glide over the greater trochanter laterally.Intra-articular snapping: Intra-articular pathology (e.g., labral tear, loose body) mimics snapping; often more harmful than extra-articular.
Up to 10% of people may notice some snapping; symptomatic cases cluster in athletes/dancers.
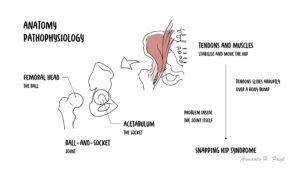
Anatomy & Physiology
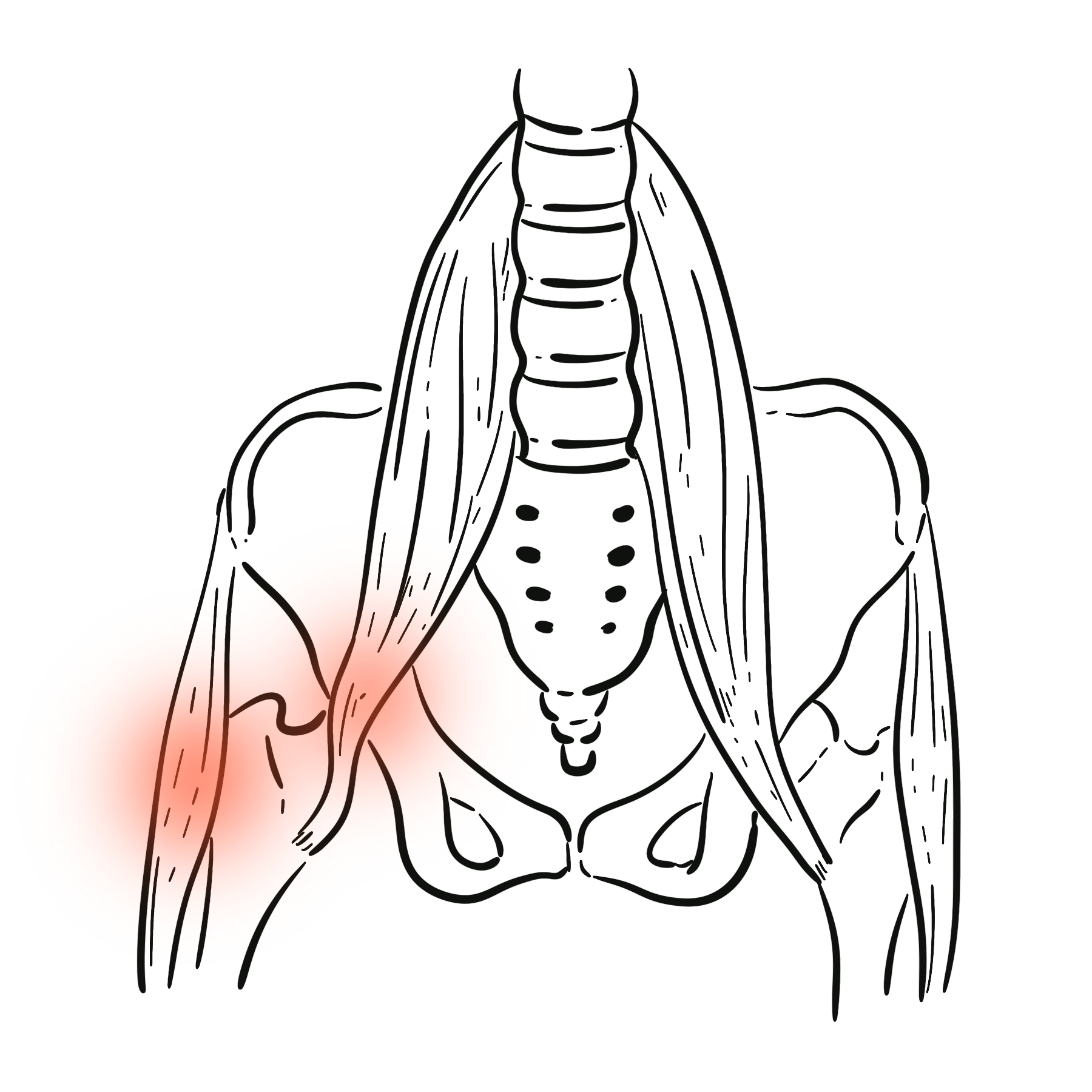
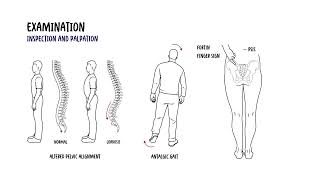
Hip joint: ball-and-socket (femoral head—acetabulum) with strong capsuloligamentous stabilizers (iliofemoral, pubofemoral, ischiofemoral) guiding motion arcs.
Iliopsoas complex: psoas major + iliacus merge to a tendon inserting at the lesser trochanter; primary hip flexor; glides across the anterior hip capsule and iliopectineal eminence.
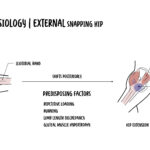
Iliotibial band (ITB): longitudinal fascia from tensor fasciae latae/gluteus maximus to Gerdy’s tubercle; passes over the greater trochanter laterally.
Labrum: fibrocartilaginous rim that deepens the acetabulum and contributes to a fluid seal and joint stability.
Dynamic stabilizers: gluteus medius/minimus (abductors), deep rotators, and core musculature coordinate pelvic control and track the femur under load
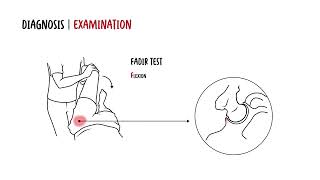
Understanding tendon paths (iliopsoas anteriorly, ITB/gluteus maximus laterally) explains where patients localise the snap and which maneuvers reproduce it.
Coexisting intra-articular disease (>50% in some iliopsoas series) is common—screen hips with persistent pain.
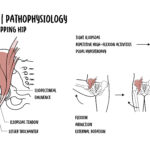
Pathophysiology
Load exposure: repetitive flexion/extension or extreme ROM → increased tendon excursion over bony/ capsular prominences.
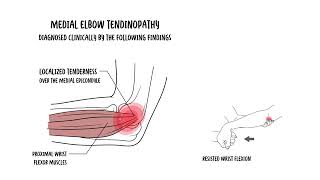
Tendon-bone interface friction: iliopsoas (anterior) or ITB/gluteus maximus (lateral) transiently “catches”—audible/palpable snap produced.
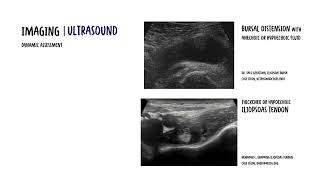
Local tissue response: peritendinous irritation ± bursal inflammation (iliopsoas or trochanteric bursa).
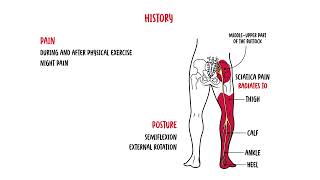
Pain generation: nociception from irritated bursa/tendon; if intra-articular pathology exists (labrum/FAI), symptoms are often more persistent and deeper.
Chronicity: motor-control adaptations (overactivity of hip flexors; abductor weakness) sustain symptoms; technique faults perpetuate snapping.
This image series is only available to members
Audible snapping without pain is common; treat the pain generator (bursa/tendon/intra-articular) rather than chasing the sound.
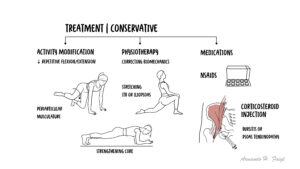
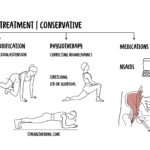
Targeted rehabilitation (first-line): iliopsoas and ITB flexibility (gentle, symptom-free stretch), progressive strengthening of abductors/extensors/core, motor-control to improve pelvic stability and femoral tracking
Image-guided injections: ultrasound-guided iliopsoas or trochanteric bursa corticosteroid/local anesthetic for diagnostics and short-term symptom control; consider for recalcitrant cases or to facilitate rehab.
Surgery (reserved)
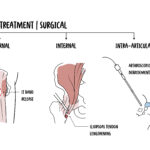
endoscopic iliopsoas fractional lengthening (internal SHS) or ITB/gluteus maximus release (external SHS) when ≥3–6 months of structured non-operative care fails
arthroscopy for intra-articular pathology ± capsular management if FAIS/labral pathology present.
Persistent pain and functional limitation due to bursitis/tendinopathy; recurrent snapping.
After iliopsoas tenotomy: transient hip-flexion weakness, possible instability (especially with dysplasia/over-resection or large capsulotomy), rare heterotopic ossification.
Most symptomatic extra-articular cases improve with education, load modification, and targeted rehab ± injection.
Poorer prognostic indicators: concomitant intra-articular pathology (labrum/FAIS), high-demand sport with extreme ROM, structural dysplasia, long symptom duration, and failure to address motor-control deficits.
Radiopaedia. Snapping hip syndrome (Radiology reference). Updated 2025. (Radiopaedia)
Wong L, et al. Understanding and Treating the Snapping Hip. Sports Med Arthrosc Rev. 2015;23(4):194-199. (Lippincott Journals)
AJR Expert Panel. Dynamic Ultrasound for Snapping Hip Syndrome (video article). AJR Am J Roentgenol. 2021. (AJR Online)
Roy A, et al. The Use of Diagnostic Musculoskeletal Ultrasound for the Iliopsoas in the Anterior Hip. Int J Sports Phys Ther. 2024;19(5):xxx-xxx. (ijspt.scholasticahq.com)
Kivlan BR, et al. External Snapping Hip Syndrome Endoscopic Treatment: “Fan-like” ITB Release. J Exp Orthop. 2020;7:xx-xx. (ScienceDirect)
Del Torto M, et al. Endoscopic release of internal snapping hip: review of literature. Muscles Ligaments Tendons J. 2016;6(3):372-377. (mltj.online)
Li J, et al. Arthroscopic/endoscopic techniques for iliopsoas release: outcomes and complications. Int Orthop. 2024;48:xxx-xxx. (SpringerLink)
Di Donato SL, et al. Diagnosis & Management of Snapping Hip Syndrome: comprehensive review. Rheumatology (Sunnyvale). 2018;8:228. (Longdom)
Lategan R, et al. Balance and strength in nonprofessional dancers with snapping hip: a cross-sectional study. SAJRSPER. 2025;47(2):e569. (journals.nwu.ac.za)
Fahey M, et al. Ultrasound-Guided Iliopsoas Bursal Injections for Iliopsoas Tendinitis after THA. J Arthroplasty. 2023;38(12):Sxxx-Sxxx. (arthroplastyjournal.org)
Morton G. Painful snapping hip due to bifid iliopsoas tendon with labral tear (case). SA J Radiol. 2015;19(1):e741. (SciELO)
Morgan P, et al. Practical office ultrasound for the hip surgeon: current concepts. J Clin Orthop Trauma. 2020;11(Suppl 2):S243–S252. (ScienceDirect)









Discussion