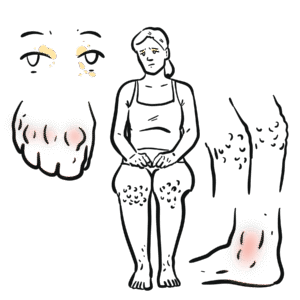
0:00 Hello, in this video we're going to talk about Addison's disease. 0:10 When you think of Addison's disease, just think of it as being opposite to C 0:14 ushing's 0:15 disease. 0:16 However, it's more that Addison's disease is characterized by insufficiency of 0:23 all the 0:23 hormones produced by the adrenal cortex. 0:29 So before going into Addison's disease it's important to revise the anatomy and 0:35 the physiology 0:36 of the endocrine system as well, more so focusing on the adrenal cortex and its 0:43 hormones. 0:45 So here we have the brain. 0:47 Within the brain is an important endocrine area called the hypothalamus. 0:52 The low-the hypothalamus are the pituitary glands made up of the anterior and 0:58 posterior 0:58 pituitary glands. 1:01 In this part we're only going to focus on the anterior pituitary gland. 1:07 Here I am depicting circulation, which is the blood, and here is one adrenal 1:14 gland. 1:15 We have two adrenal glands sitting above two kidneys. 1:20 The adrenal glands has a cortex, the outer part of the adrenal gland, and it 1:24 has the 1:25 medulla, which is the inner part. 1:28 The adrenal gland produces hormones in response to the brain, specifically in 1:34 response to 1:35 the hypothalamic pituitary axis. 1:39 The hypothalamus produces a hormone called corticotropic releasing hormone. 1:46 Cortic releasing hormone stimulates cells within the anterior pituitary gland 1:53 to secrete 1:54 adenocorticotropic stimulating hormone, or ACTH for short. 2:00 ACTH will then enter circulation. 2:03 ACTH will then travel towards the adrenal glands, specifically the adrenal 2:09 cortex, where it 2:10 will stimulate the adrenal cortex to produce and secrete hormones. 2:15 The hormones produced by the adrenal cortex are three, and they are categorized 2:20 as mineral 2:21 corticoids, such as aldosterone, glucocorticoids, such as cortisol, and and 2:30 rogens. 2:31 It's important to note that androgen secretion from the adrenal cortex has 2:37 minimal role in 2:38 males. 2:39 Rather, it has more of an important role in females. 2:45 Hydrogen in men are mainly produced by the testes. 2:49 An increase in cortisol and circulation will have a negative feedback on the 2:55 hypothalamus. 2:56 It will tell the hypothalamus to stop producing any more corticotropin-re 3:01 leasing hormone, thus 3:02 decreasing the stimulation of adrenal cortex hormone production. 3:09 So what do these adrenal cortex hormones actually do? 3:12 What does the mineral corticoids, glucocorticoids, and androgens do exactly? 3:19 Well mineral corticoids, mainly aldosterone, has a function to increase sodium 3:25 and water 3:25 retention in a body, and they primarily work on the kidneys. 3:31 And so they retain sodium and water, resulting in an increase in blood pressure 3:39 . 3:40 Glucocorticoids, such as cortisol, does many things. 3:43 The effects are usually long-term, and is often referred to as the stress 3:51 response. 3:53 Effects of cortisol include immunosuppression, and because it is immunosupp 3:58 ression it is 3:59 also an anti-inflammatory. 4:02 This also means that infection risk increases. 4:08 Glucocorticoids has a profound effect on metabolism. 4:11 It causes weight gain and insulin resistance. 4:15 Glucocorticoids causes skin thinning, and in the bone, glucocorticoids 4:20 stimulates osteoclastic 4:21 activity, which are the bone eating cells, resulting in an increase in osteopen 4:28 ia and 4:28 osteoporosis, which is bones with low mineral density, increasing the risk of 4:35 bone fractures. 4:36 Finally, cortisol itself has an effect on blood pressure, which will increase 4:41 the blood 4:42 pressure. 4:44 The androgen secreted by the adrenal glands, as mentioned earlier, has more of 4:50 an effect 4:51 on females. 4:53 From what we have learned, we can see that the adrenal glands have a big role 4:58 in maintaining 4:59 our body's homeostasis. 5:02 Another production of the adrenal cortex hormones can cause big problems, but 5:08 also underproduction 5:09 of adrenal cortex hormones can have severe consequences. 5:13 Addison's disease is essentially any cause of primary adrenal cortex insuff 5:20 iciency, or 5:20 in other words, a decrease in production of adrenal cortex hormones. 5:26 So let's look at some examples. 5:31 Even here we have the brain, we have the main structure to focus on, the 5:35 hypothalamus and 5:36 the anterior pituitary gland. 5:38 Here is the circulation. 5:41 The adrenal glands have receptors on them. 5:44 Here I am drawing a receptor on the adrenal cortex. 5:48 The hypothalamus releases corticotropin-releasing hormone, which stimulates the 5:52 anterior pituitary 5:54 gland to produce adenocorticotropic hormone, or ACTH for short. 6:00 ACTH goes into circulation and stimulates the adrenal cortex, as mentioned 6:06 earlier. 6:07 The main cause of primary adrenal insufficiency, and therefore the main cause 6:12 of Addison's 6:13 disease, are antibodies being produced against adrenal cortex cells, as well as 6:21 plus minus 6:22 21 hydroxylase enzyme within the adrenal gland. 6:28 And these antibody production actually accounts for 70% of cases of Addison's 6:34 disease. 6:35 The O2 immune attack of the adrenal cortex causes damage, and therefore reduces 6:40 the production 6:41 of the mineral corticoids, glucocorticoids, and androgens. 6:48 A decreased production of mineral corticoids will cause a reduction of sodium 6:53 and water 6:53 retention, and so will reduce the blood pressure. 6:57 A decrease in blood pressure will cause tachycardia as a compensatory mechanism 7:03 . 7:03 A reduction in androgens does not really have an effect on males, rather more 7:08 of an 7:08 effect on females, causing a decrease in libido. 7:14 A reduction of the glucocorticoids by the autoimmune attack causes many things. 7:19 Basically the opposite effects of what glucocorticoid steroids would otherwise 7:24 do. 7:24 This means that people with Addison's disease will have weight loss, skin pig 7:31 mentation, 7:32 and fatigue in general. 7:34 Further, because there is a decrease in glucocorticoids, this means the 7:41 negative feedback is off. 7:44 Remember, negative feedback only occurs when there is an increase in hormone 7:48 levels in 7:49 the blood. With no negative feedback by the glucocorticoids or cortisol, the 7:55 hypothalamus 7:56 will produce more corticotropic releasing hormone, and therefore stimulate the 8:01 anterior 8:02 pituitary to produce more adrenocorticotropic hormone. 8:07 The increase in corticotropic releasing hormone will actually stimulate other 8:13 hormones produced 8:14 by the pituitary gland, including prolactin. 8:20 So now the question is, what are the effects of having reduced adrenal cortex 8:24 hormone levels? 8:26 What are the effects on our body? 8:29 Clinical presentation. 8:31 As we have learned, Addison's disease is essentially primary adrenal insuff 8:38 iciency, and so the 8:39 clinical presentation includes tiredness, dizziness and nausea, weight loss, 8:47 vomiting 8:48 diarrhea, abdominal pain, hyperpigmentation, which is generalized, decreased 8:56 libido, which 8:57 is mainly in female, arthralgia and myalgia. 9:04 On clinical examination, there will be a low grade fever, signs of dehydration 9:09 and loss 9:10 of hair. 9:13 You can also note picaxia as well as postural hypotension, which is a decrease 9:19 in blood 9:19 pressure, the difference between lying down and standing up. 9:25 Finally, tachycardia is also present to compensate for the low blood pressure. 9:32 Let's go back to the main diagram again. 9:36 As mentioned, O2 antibodies against the adrenal cortex and the enzyme 21 hydrox 9:42 ylase accounts 9:42 for 70% of Addison's disease cases. 9:46 However, there are other causes, including infections, adrenal cortex malign 9:55 ancy, secondary 9:56 malignancy of the adrenal cortex from metastasis elsewhere, such as the lungs, 10:04 adrenal cortex 10:05 hemorrhage or infarction. 10:09 The patient might be on warfarin, which predisposes them to this. 10:16 Addison's disease can be caused by infiltration diseases, such as hemochromat 10:21 osis and amyloidosis. 10:23 There are also eatrogenic causes, such as removal of the adrenal glands, which 10:28 will 10:28 obviously cause a reduction in the adrenal cortex hormones. 10:35 A rare congenital cause is characterized by ambiguous genitalia, and this is 10:42 known as congenital 10:43 adrenal hyperplasia. 10:45 Finally, medications that can cause a decrease in cortisol production can cause 10:52 Addison's. 10:53 This includes itomidate, mitotane, and amino glutathymide. 11:01 Some of these drugs of which are usually used to treat Cushing syndromes. 11:09 Risk factors for Addison's disease include female gender, because most 11:14 autoimmune diseases 11:15 actually tend to occur in females. 11:18 Having an autoimmune disease, adrenal cortex autoantibody production, adrenal 11:25 hemorrhage 11:26 is another risk factor, tuberculosis infection, meningococcal infection with 11:33 adrenal hemorrhage, 11:34 and of course, using medications that can induce Addison's disease is a risk 11:40 factor. 11:41 Recapping primary adrenal insufficiency is Addison's disease, which has 11:48 multiple many 11:48 causes. 11:51 Secondary adrenal insufficiency is caused by hypothylamic or pituitary 12:01 dysfunction. 12:04 Investigations into Addison's disease. 12:07 In Addison's disease, there is reduced production of mineral corticoids and 12:12 decreased production 12:13 of glucocorticoids. 12:15 However, because of low amounts of glucocorticoids, as we learned, negative 12:20 feedback does not 12:21 occur, and so there is an increase in ACTH production by the anterior pituitary 12:28 gland. 12:29 Investigations to be performed include checking serum ACTH, which will show an 12:35 increase in 12:36 serum ACTH, and also checking for the presence of adrenal autoantibodies. 12:43 There will be an increase in serum cortisol. 12:46 Other blood tests include full blood count and performing EUC, which may show 12:53 hyponaturmia, 12:55 perchlemia, and increase inuria. 12:59 Finally, imaging such as CT scan is important, which may reveal adrenal tumours 13:05 or adrenal 13:06 hemorrhage. 13:08 A thyroid function test is also important, as one of the main differentials for 13:13 Addison's 13:13 disease is Graves' disease. 13:18 Management of Addison's disease. 13:20 The most important part is to educate the patient, particularly to never miss a 13:26 dose of medication, 13:28 and we will learn the reason why. 13:34 The medications for Addison's disease include replacing the hormones, which are 13:40 lost. 13:41 This means using glucocorticoid replacements, such as hydrocortizone. 13:47 Alcoholocorticoid replacements, such as fluidrocortizone. 13:52 And this will replace diminished endogenous menocorticoid production. 14:00 Androgen replacement are mainly for females. 14:03 Finally, for management, monitoring is important, because of the complications 14:09 associated with 14:10 Addison's disease, but mainly also because of the medication used as well. 14:16 Too much glucocorticoids replacement can cause secondary cushions. 14:22 It can also cause osteopenia and osteoporosis, increasing the risk of bone 14:29 fractures. 14:30 Mineral cocorticoids and glucocorticoid replacement can also cause secondary 14:36 hypertension. 14:37 But most serious complication is adrenal crisis, which is where there is a 14:43 sudden drop 14:43 in glucocorticoid levels. 14:46 This is often caused when patients on long-term glucocorticoids suddenly stop 14:52 taking the glucocorticoid 14:53 replacement, or because they are not taking enough glucocorticoids. 14:59 In general, what happens, the patient on long-term glucocorticoids will 15:05 increase glucocorticoid 15:07 levels, which will have a negative feedback on the hypothalamus. 15:13 And so because of this negative feedback, there will be a decrease in ACTH. 15:21 And remember, in patients with Addison's disease, the adrenal cortex does not 15:26 work properly. 15:27 They don't produce enough glucocorticoids. 15:31 Especially now with the reduced ACTH, the little remaining functional part of 15:38 the adrenal 15:38 cortex will not produce anything and just atrophy and become non-functioning. 15:46 And so if all of a sudden glucocorticoid replacement therapy is stopped, there 15:52 will 15:52 literally be no adrenal cortex hormones, and this is essentially a adrenal 15:59 crisis. 16:00 And so patient education is vital. 16:03 It's important to not miss doses, encourage them to wear a mobile bracelet. 16:08 And third point, double the dose of glucocorticoids during febrile illness, or 16:13 during periods 16:14 where it is necessary.