

Long-Term Complications of Diabetes (Overview)
Overview
Classification
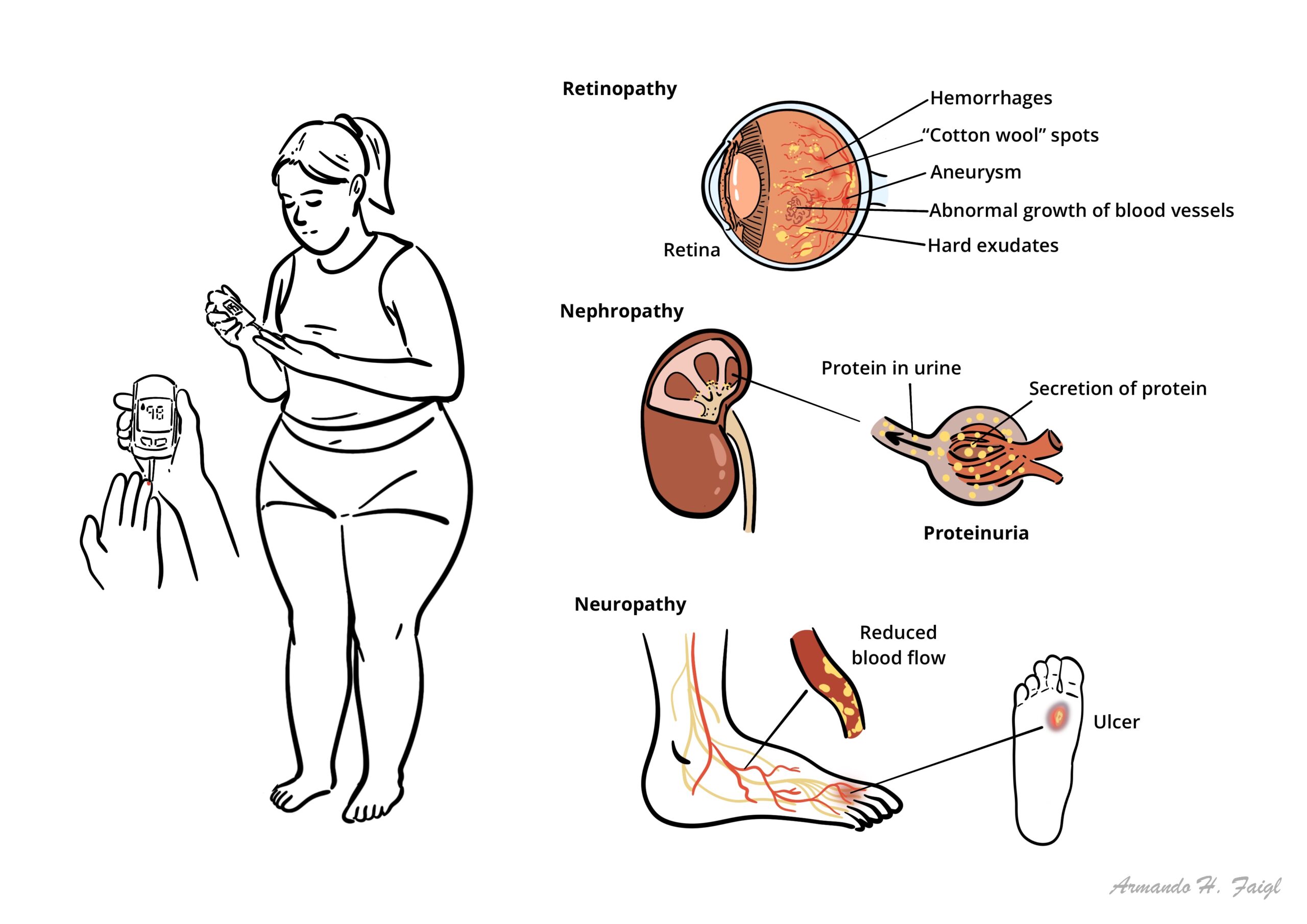
- Microvascular Complications
- Retinopathy
- Nephropathy
- Neuropathy
- Macrovascular Complications
- Coronary heart disease
- Cerebrovascular disease
- Diabetic foot
Diabetic Retinopathy
Overview
Diabetes is the most common cause of blindness in the working population. Blindness is preventable. Annual retinal screening is advised for patients at risk. Pre-symptomatic screening enables laser photocoagulation to be used, aimed to stop production of angiogenic factors from the ischaemic retina.
The fundus are usually bilateral and broadly symmetrical.
Findings depend on severity and are classified into:
- Non-proliferative
- Proliferative
- Diabetic maculopathy
Non-proliferative diabetic retinopathy
- Cotton wool spots (infarcts)
- Microaneurysms (dots)
- Haemorrhages (spots)
- Venous beading
- Hard exudates (lipid deposits)
- Severe (4:2:1 rule) – haemorrhages or microaneurysms in all 4 quadrants. Venous beading in 2 or more quadrants. Intraretinal microvascular abnormalities in at least 1 quadrant.
Proliferative diabetic retinopathy
- New vessels form (proliferation)
- This needs urgent referral

Diabetic maculopathy
- Hard to see in early stages, suspect if acuity decreased
- Macular/retinal Oedema
| Risk Factors for worsening retinopathy |
| Duration of diabetes |
| Type 1 diabetes |
| Hypertension |
| Poor diabetic control |
| Diabetic nephropathy |
| Pregnancy |
| Alcohol/Smoking |
Diabetic Nephropathy
Overview
Type II diabetes Mellitus is the leading cause of Chronic Kidney Disease. It is classified as a secondary nephrotic syndrome. ~10% of will people will have nephropathy at diagnosis and up to half will go on to develop it over the next 20yrs. 20% of people with Type II diabetes will develop end stage kidney disease. Everyone with Diabetes should be screened yearly for microalbuminuria.
Clinical features – Nephrotic Syndrome with signs and symptoms of diabetes (hyperglycemia)
More info on Nephrotic Syndrome
Pathological features Diabetic kidney disease is defined by characteristic structural and functional changes. The predominant structural changes include
- Mesangial expansion
- Glomerular basement membrane thickening
- Glomerular sclerosis
| Staging | |
| Class I | Isolated glomerular basement membrane thickening. There is no evidence of mesangial expansion, increased mesangial matrix, or global glomerulosclerosis involving >50 percent of glomeruli. |
| Class II | Mild (class IIa) or severe (class IIb) mesangial expansion. |
| Class III | At least one Kimmelstiel-Wilson lesion (nodular intercapillary glomerulosclerosis) is observed on biopsy and there is <50 percent global glomerulosclerosis. |
| Class IV | Advanced diabetic sclerosis. There is >50 percent global glomerulosclerosis. |
Management and Prognosis – Microalbuminuria is reversible if caught early and managed vigorously:
- Tight glycemic control
- Right BP control with ACE/ARBs
- Manage cardiovascular disease risk factors
More info on Chronic Kidney Disease
Diabetic Neuropathy
Overview
Involvement of the peripheral and autonomic nervous systems is probably the most common complication of diabetes. The high rate of diabetic neuropathy results in substantial morbidity, including recurrent lower extremity infections, ulcerations, and subsequent amputations
Classification
Symmetric polyneuropathy
Characterized by a progressive loss of distal sensation correlating with loss of sensory axons, followed, in severe cases, by motor weakness and motor axonal loss. Classic “stocking-glove” sensory loss, tingling and pain (worse at night).
Autonomic neuropathy
It is a diagnosis of exclusion and may be unnoticed because of multiorgan involvement and insidious onset. Problems that can occur are postural hypotension, gastroparesis, urine retention, erectile dysfunction and constipation or diarrhoea.
Gastroparesis is characterised by early satiety, post-prandial bloating and nausea/vomiting. It is diagnosed by gastric scintigraphy with a technutium labelled meal.
Mononeuropathies
- Cranial – CN III, CN IV and CN VI affected causing ptosis, diplopia and pain around the area
- Peripheral – Median nerve around the wrist neuropathy, foot drop (perineal nerve palsy)
- Mononeuritis multiplex (both cranial and peripheral involvement)
Diabetic amyotrophy
include the acute, asymmetric, focal onset of pain followed by weakness involving the proximal leg, with associated autonomic failure and weight loss.
Diabetic Foot
Overview
The high rate of diabetic neuropathy results in substantial morbidity, including recurrent lower extremity infections, ulcerations, and subsequent amputations. The combination of peripheral vascular disease and peripheral neuropathy can lead to repeated minor trauma to the feet leading to ulceration and infection which are very slow to heal. Examine foot regularly.
Clinical features
Typically painless, punched out ulcer in an area of thick callus +/- superadded infection. This can then lead to cellulitis, abscess +/- osteomyelitis.
To examine foot regularly. Distinguish between ischaemia (absent foot pulses) and peripheral neuropathy (↓sensation in stocking distribution, absent ankle reflex, charcot’s joints). Many have both ischaemic and neuropathic changes.
Assess degree of:
- Neuropathy (clinically)
- Ischaemia (clinically + doppler +/- angiography)
- Bone deformity – charcot’s joint (clinically + x-ray)
- Infection (swabs, blood culture, x-ray for osteomyelitis, probe ulcer to reveal depth)
- Early referral
- Multidisciplinary teams
- Little evidence that any dressing for an ulcer is superior
- Primary consideration → exudate management → maintain moisture balance
- Secondary consideration
- Facilitating autolytic debridement (for necrotic or sloughy tissue)
- Wound depth (e.g. need to fill cavity)
- Bacterial management → antibiotics
- Signs of infection
- Temperature
- Would-related pain → analgesia
In cases of infections the common organisms are staphs, streps, anaerobes. Treat with IV benzylpenicillin and flucloxacillin +/- metronidazole
More info on lower limb ulcers
Pharmacology
Metronidazole inhibits nucleic acid synthesis in microbes, more effective against anaerobic microorganisms. Side effects: nausea, diarrhoea, weight loss, abdominal pain, vomiting, headache, dizziness, metallic taste in the mouth. Rarer side effects: thrombophlebitis, leukopenia, neutropenia and peripheral neuropathy.
Pathogenesis
It is the vascular changes in diabetes that leads to the complications. High blood glucose causes endothelial changes causing increased production of reactive oxygen species (ROs), growth factors (VEGF, cell growth factors), toxic metabolites and cytokines. The production of these substances promotes atherosclerosis, arteriosclerosis causing ischaemic changes. The metabolic toxins together with the ischaemic changes lead to the microvascular and macrovascular changes seen in diabetes.







Members only discussions coming soon…