

Anaphylaxis

Overview
Anaphylaxis is a severe, systemic hypersensitivity reaction that is rapid in onset and potentially fatal, most often triggered by foods, medications, or venom; global incidence is ~50–112 per 100,000 person-years with rising emergency presentations in many regions, including Australia [1,2,4].
Mortality is low but non-trivial and is driven by airway obstruction, severe bronchospasm, or distributive shock when adrenaline (epinephrine) is delayed. Risk is increased by comorbid asthma, mast cell disorders, older age, cardiovascular disease, and co-factors such as NSAIDs, alcohol, and exercise that lower reaction thresholds.
Definition
Anaphylaxis: serious, systemic hypersensitivity with rapid onset involving airway/breathing/circulation and/or typical skin–mucosal features; skin signs may be absent.
Biphasic anaphylaxis: recurrence of symptoms after initial resolution without re-exposure, typically within 1–24 h (occasionally up to 72 h); higher risk with severe initial reactions or >1 adrenaline dose.
Serum tryptase: mast-cell mediator that peaks ~1–2 h after onset and supports diagnosis when elevated above baseline; normal level does not exclude anaphylaxis.
Treat first, confirm later—do not delay adrenaline while seeking tests.
Aetiology & Risk factors
Aetiology
- IgE-mediated: foods (peanuts/tree nuts/shellfish), drugs (β-lactams, perioperative agents), insect venom; latex; allergen immunotherapy
- Non-IgE immunologic: complement-mediated or immune-complex pathways in selected drug/contrast reactions
- Non-immunologic (direct mast-cell activation): radiocontrast media, opioids, vancomycin, exercise-induced (± food), alcohol, temperature extremes
- Host: asthma (especially uncontrolled), mastocytosis/mast-cell activation disorders, older age, cardiovascular disease, pregnancy
- Medications: beta-blockers and ACE inhibitors may worsen hypotension/bronchospasm and reduce adrenaline responsiveness
- Situational co-factors: exercise, NSAIDs, alcohol, intercurrent infection, sleep deprivation; these lower the threshold for food-related reactions and amplify severity
In reactions requiring >1 adrenaline dose, anticipate severe or biphasic anaphylaxis and extend observation.
Pathophysiology
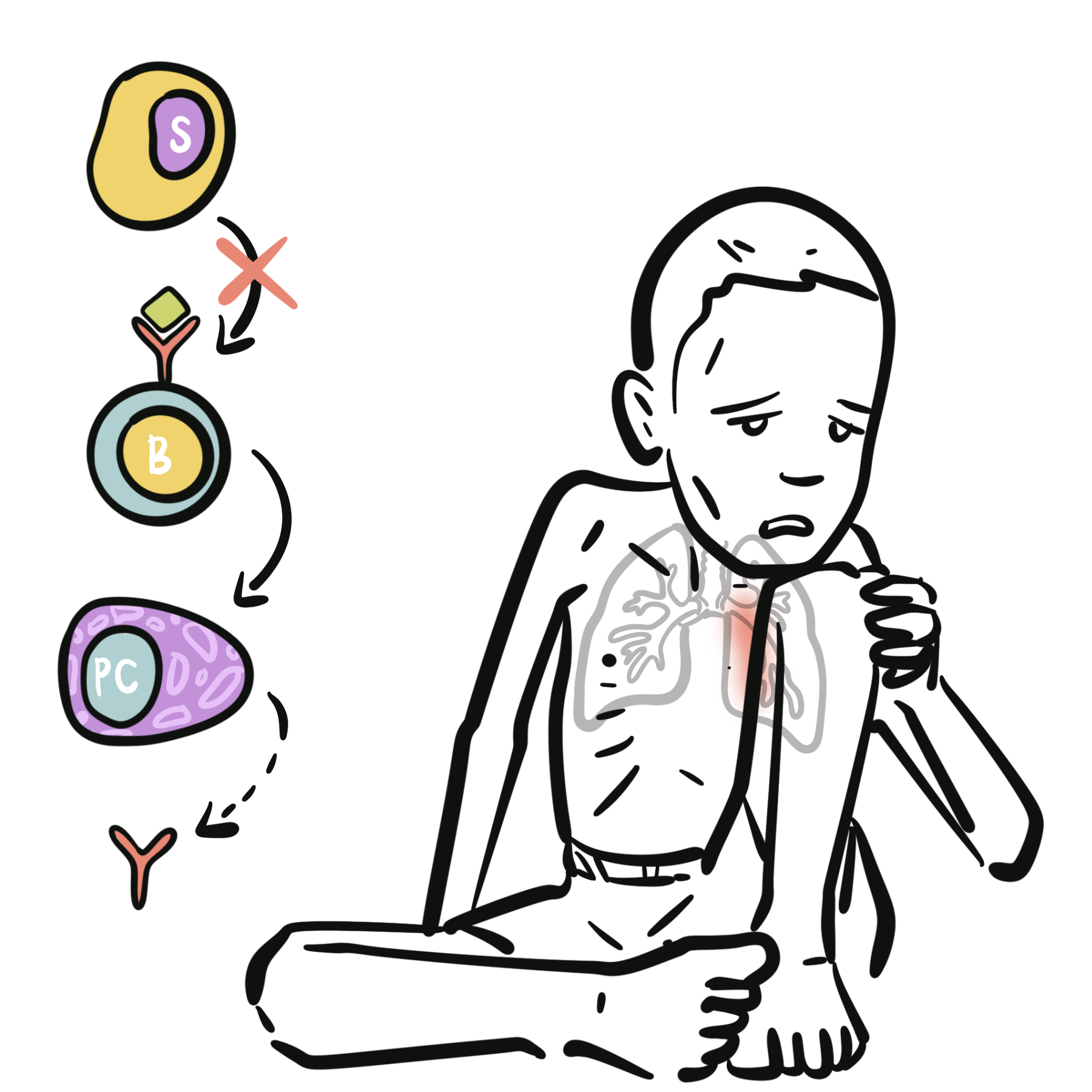
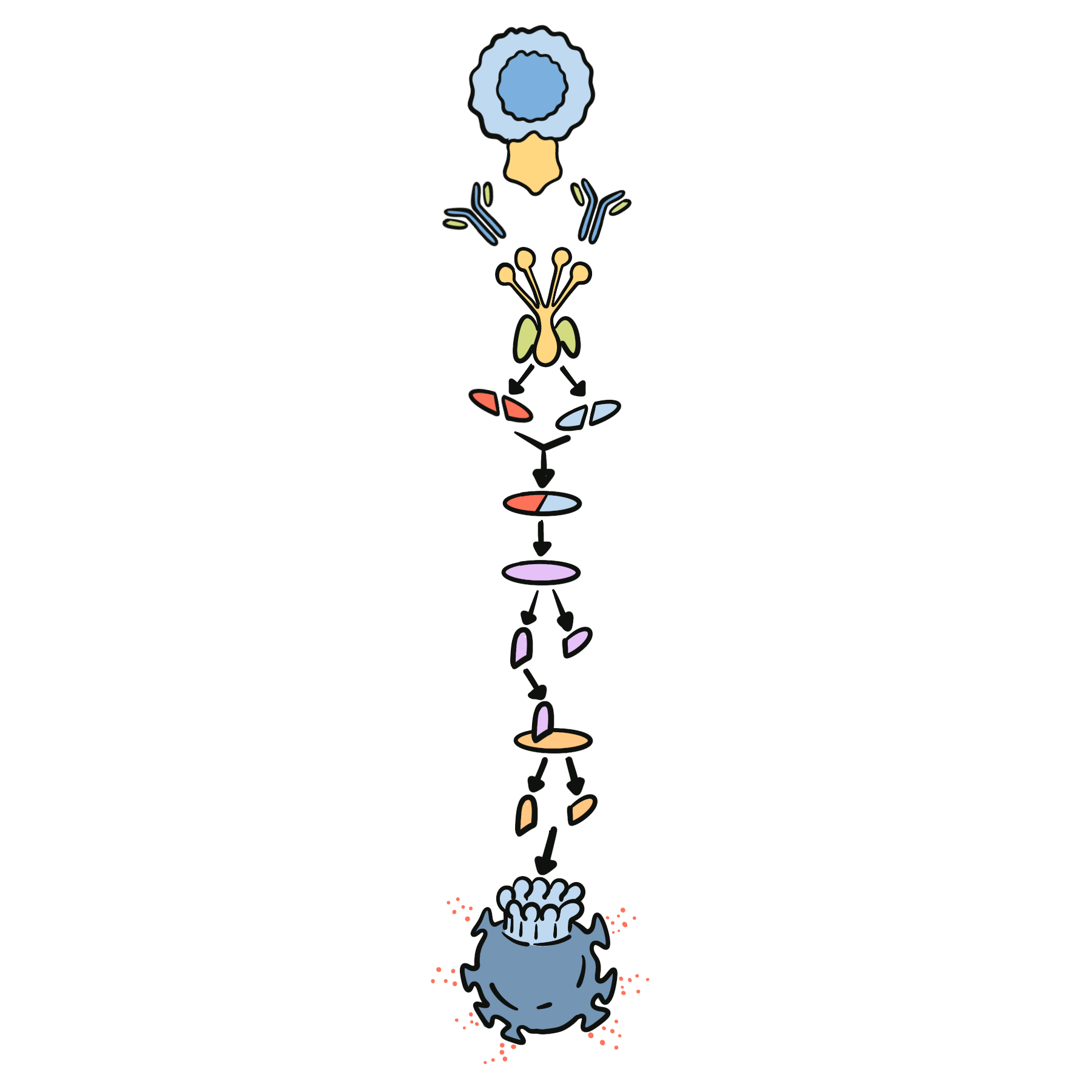
- Initial exposure to an allergen leads to antigen presentation and Th2 immune polarisation.
- IL-4 and IL-13 drive B-cell class switching to produce IgE.
- IgE binds FcεRI receptors on mast cells and basophils, causing sensitisation.
- On re-exposure, allergen cross-linking of IgE–FcεRI complexes triggers mast-cell degranulation.
- Histamine, tryptase, leukotrienes, and prostaglandins are released.
- These mediators cause vasodilation, increased vascular permeability, smooth-muscle contraction, and mucus secretion.
- Clinical effects include urticaria, angioedema, wheeze, stridor, hypotension, and possible shock.
Skin signs are absent in up to 20%—do not exclude anaphylaxis if airway/breathing/circulation are compromised after a likely exposure.
Clinical Manifestations
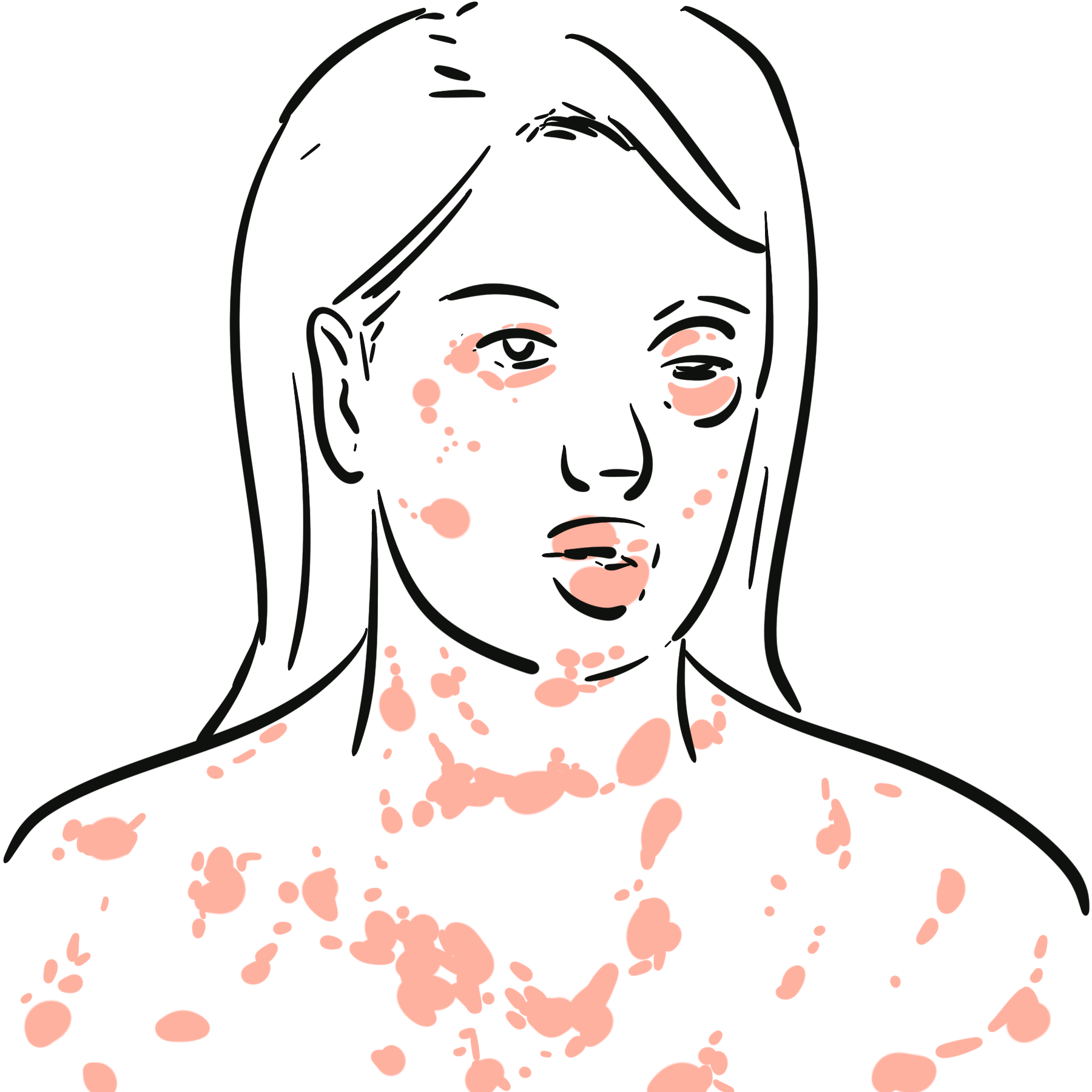
- Skin/mucosa: urticaria, flushing, pruritus, angioedema (lips/tongue/uvula), conjunctival injection; may be absent
- Respiratory: throat tightness, hoarseness/stridor, wheeze, persistent cough, dyspnea, hypoxemia
- Cardiovascular: dizziness/syncope, hypotension, tachycardia (or bradycardia with vasovagal), shock, collapse
- Gastrointestinal: crampy abdominal pain, vomiting, diarrhea (especially with food triggers)
- Neurologic: sense of doom, confusion; seizure in profound hypoxia/hypotension.
Supine positioning (left lateral if pregnant) reduces venous pooling; sudden standing can precipitate arrest in anaphylaxis.
Diagnosis
- Clinical diagnosis—use criteria to treat without delay; obtain serum tryptase 30–180 min after onset and a baseline ≥24 h later if feasible (does not delay therapy)
- Latest consensus criteria (WAO 2020; JTFPP 2023)—anaphylaxis is highly likely when any of the following are met
- Acute onset of illness with skin/mucosal involvement (urticaria/angioedema) and at least one of: respiratory compromise or reduced blood pressure/end-organ dysfunction.
- Two or more of the following after likely allergen exposure: skin–mucosal involvement; respiratory compromise; reduced blood pressure; persistent GI symptoms.
- Reduced blood pressure after exposure to a known allergen for that patient (age-specific thresholds).
Treatment
- Immediate first-line (do not delay): IM adrenaline into anterolateral mid-thigh 0.01 mg/kg (1:1000) up to 0.5 mg adult, repeat every 5–15 min if needed [1,3,4,9].
- Positioning & basic life support: lay supine (left lateral in pregnancy), high-flow oxygen, large-volume IV isotonic fluids for hypotension; attach monitoring [3,4].
- Respiratory adjuncts: salbutamol for bronchospasm; nebulised adrenaline for upper-airway edema as adjunct (not instead of IM adrenaline) [3,4].
- If on beta-blocker with refractory shock/bronchospasm: IV glucagon (e.g., 1–5 mg over 5 min then infusion) with antiemetic and monitoring [3,4].
- Adjunctive drugs (after adrenaline): H1 antihistamines for cutaneous symptoms; systemic corticosteroids not first-line and do not prevent biphasic reactions—consider only as adjunct in protracted symptoms [3,8].
- Observation: risk-stratified—minimum 4–6 h for mild responsive cases; ≥6–12 h or admit if severe, needed >1 adrenaline dose, hypotension/respiratory compromise, or significant comorbidity/late-night presentation [3,8].
- Discharge essentials
- prescribe adrenaline auto-injector(s)
- provide written action plan
- education on avoidance/risk co-factors
- allergy referral, and arrange follow-up; consider baseline tryptase and trigger work-up
Complications & Prognosis
- Airway obstruction (laryngeal edema)
- Severe bronchospasm
- Refractory shock
- Biphasic reactions
- Myocardial ischemia/arrhythmia (rare, usually with delayed treatment or IV bolus errors)
- Most episodes resolve with prompt adrenaline and supportive care; recurrence risk depends on trigger control and patient education; delayed adrenaline, severe initial reaction, need for >1 dose, unknown trigger, and comorbid asthma predict biphasic/severe courses [3,8].
References
- Cardona V, Ansotegui IJ, Ebisawa M, et al. World Allergy Organization anaphylaxis guidance 2020. World Allergy Organ J. 2020;13(10):100472. (worldallergyorganizationjournal.org)
- ASCIA. Guidelines: Acute management of anaphylaxis. 2024 update. Available from ASCIA website. (Allergy Australia)
- Golden DBK, Wang J, Lieberman JA, et al. Anaphylaxis: A 2023 practice parameter update. Ann Allergy Asthma Immunol. 2024;132(2):121–152. (Ann Allergy)
- Muraro A, Worm M, Alviani C, et al. EAACI guidelines: Anaphylaxis (2021 update). Allergy. 2022;77(2):357–377. (PubMed)
- Shin M, Lee S. Food allergies and food-induced anaphylaxis: role of cofactors. Clin Exp Pediatr. 2021;64(8):389–395. (PMC)
- Bartra J, et al. Cofactors in food anaphylaxis in adults. Ann Allergy Asthma Immunol. 2023;131(3):343–350. (Ann Allergy)
- Muñoz-Cano R, et al. Effect of cofactors in basophils and mast cells. Front Immunol. 2021;12:623071. (Frontiers)
- Shaker MS, Wallace DV, Golden DBK, et al. Anaphylaxis—2020 practice parameter update: biphasic risk and observation. J Allergy Clin Immunol. 2020;145(4):1082–1123. (JACI)
- NSW Agency for Clinical Innovation. Adult ECAT protocol: Anaphylaxis. 2023. (Agency for Clinical Innovation)
- Frith K. Adrenaline injector devices: a 2024 update on prescribing. Medicine Today. 2024;25(10). (Medicine Today)


Members only discussions coming soon…