

Carotid Artery Disease
Overview
Carotid artery disease refers to atherosclerotic narrowing of the carotid artery lumen. It is associated with approximately 10-15% of all ischaemic strokes. Stroke is the third leading cause of death and a principal cause of long-term disability in much of the industrialised world. The degree of internal carotid artery stenosis is the most important predictor of cerebral infraction among patients with extracranial carotid artery disease.1
Definition
Stroke: Acute onset of neurological dysfunction due to brain tissue infarction, caused by disturbance of blood flow to the brain. Strokes are mainly categorised into ischaemic and haemorrhagic.
Transient Ischaemic Attack (TIA): Minor stroke characterised by a brief episode of neurological dysfunction caused by focal cerebral ischaemia without infarction. Symptoms resolve in <24 hours and there is no evidence of infarction on imaging.
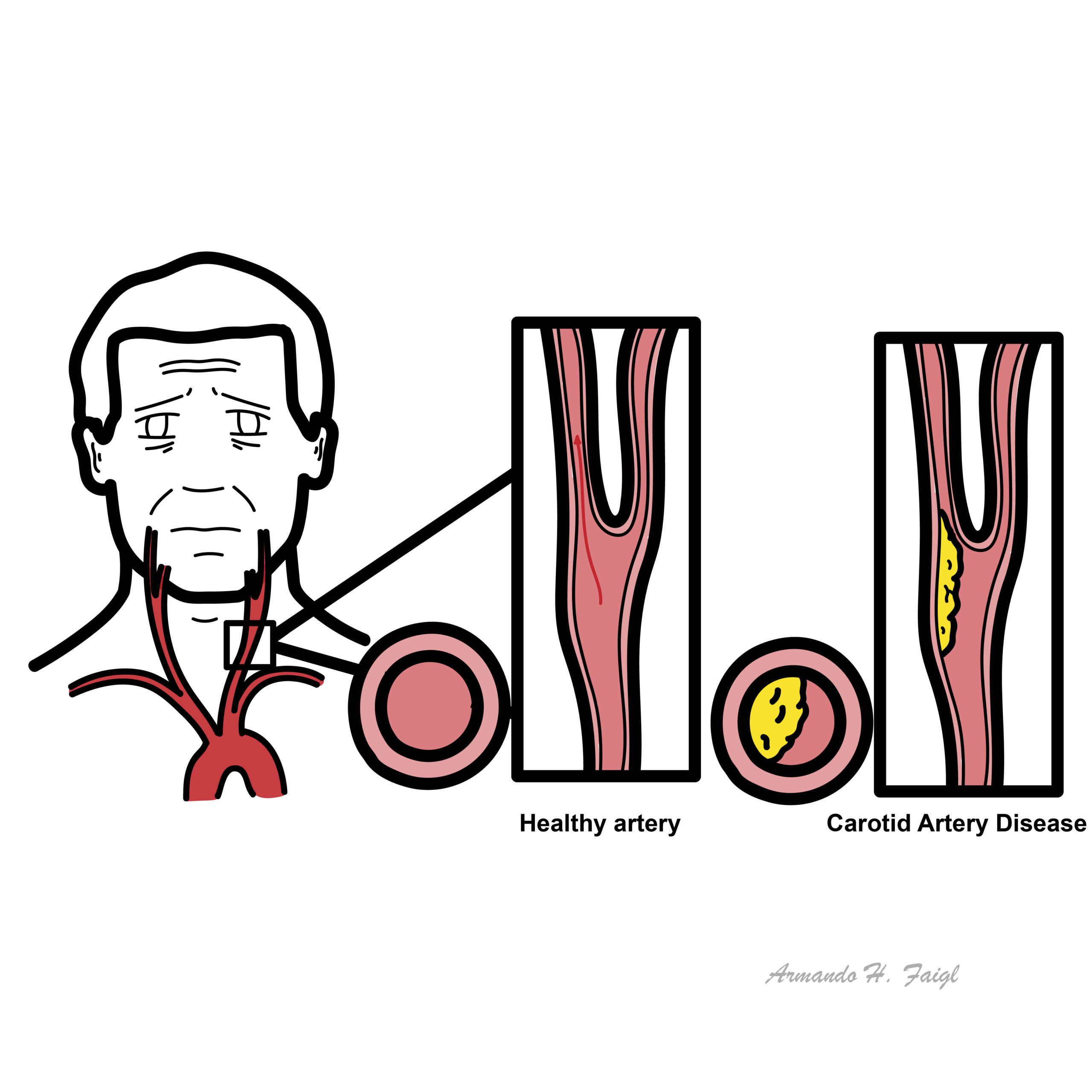
Atherosclerosis: Progressive disease characterised by the accumulation of lipids and fibrous elements in large arteries (plaque).
Carotid artery stenosis: Typically the result of atherosclerosis at the bifurcation of the common carotid artery or in the origins of either the internal or external carotid artery.
30% of patients who present with suspected stroke have a ‘stroke mimic’ such as tumour, subdural haematoma, migraine, hypoglycaemia, postictal paralysis or cerebral abscess.
Initial mortality of an ischaemic stroke ranges from 15-30%. Survivors remain at a high risk of subsequent stroke (50% of patients will experience a second event in 5 years).
Anatomy
Common Carotid
Origin:
- Left common carotid: Aortic Arch
- Right common carotid: Brachiocephalic trunk of Aortic Arch
Common carotid arteries bifurcate variably at the C3/4 or C4/5 and give rise to internal carotid and external carotid.
External Carotid
Branches (from proximal to distal) – Some Anatomists Like Freaking Out Poor Medical Students:
- Superior Thyroid
- Ascending Pharyngeal
- Lingual
- Facial
- Occipital
- Posterior Auricular
- Maxillary
- Superficial Temporal
Internal Carotid
Important branches:
- Superior and Inferior Hypophyseal arteries – supply the pituitary gland
- Ophthalmic artery – supplies the eye
- Posterior Communicating – connects Internal Carotid and Posterior Cerebral
Terminates into: Anterior Cerebral and Middle Cerebral.
Carotid Sheath
Condensation of the deep cervical fascia that surrounds the great vessels of the neck
Contains:
- Internal Jugular vein
- Vagus nerve
- Common Carotid or Internal Carotid (depending on vertebral level observed)
Carotid body – cluster of chemoreceptor cells located at the bifurcation
Carotid sinus – dilation at the bifurcation and proximal aspect of internal carotid that contains baroreceptors.
Aetiology and Risk factors
- Advancing age
- Male gender
- Smoking
- Family history
- Atherosclerosis
- Hypertension
- Hypercholesterolaemia
- Other vascular aneurysm
Pathophysiology
The pathophysiology of cerebrovascular disease (stroke or TIA) can be of:
- Intracranial origin
- Extracranial origin
- Flow-restrictive lesions – carotid artery stenosis most common
- Embolism
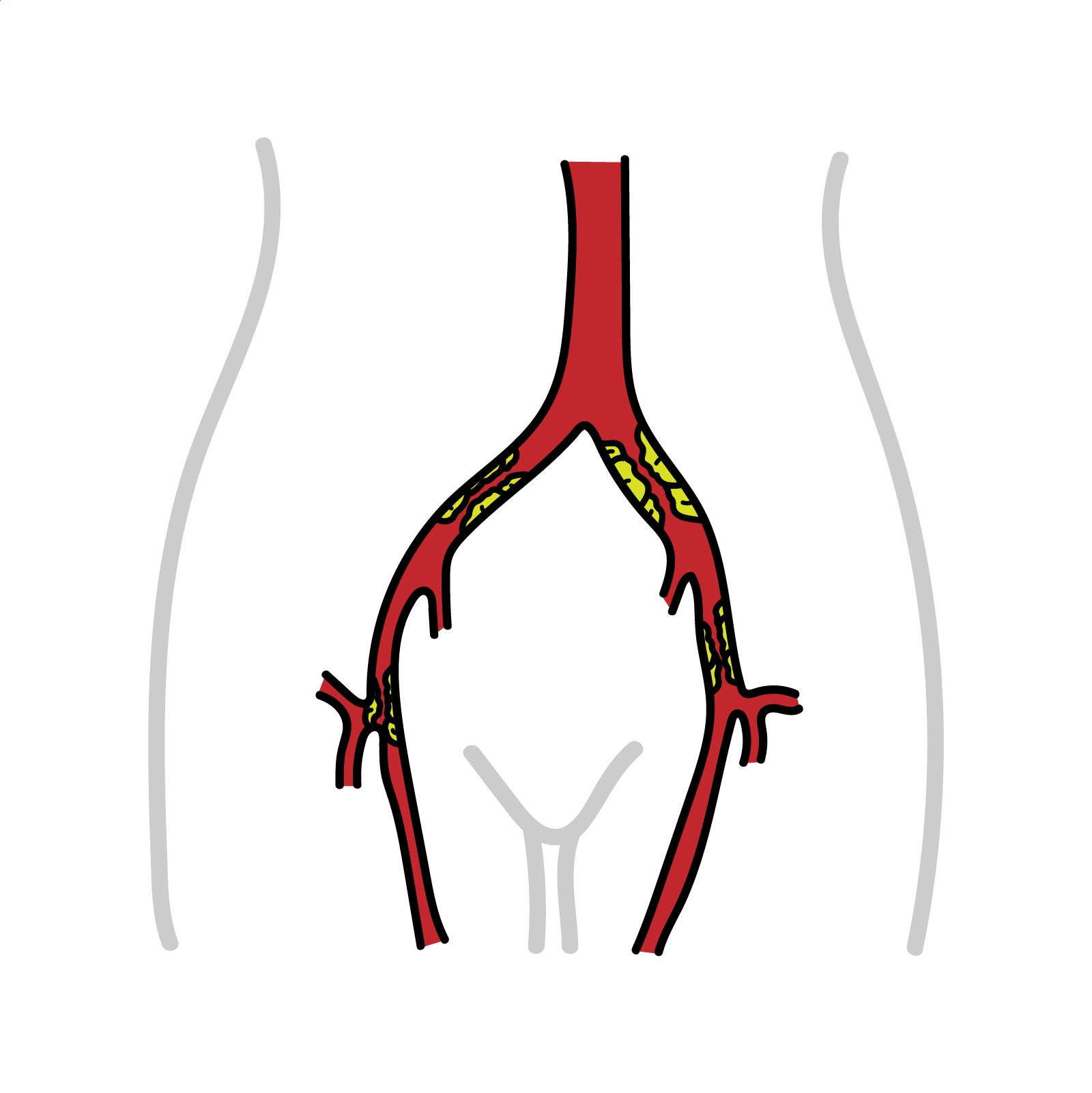
Carotid Artery Stenosis pathophysiology
- Atherosclerosis formation in carotid artery at areas of turbulent flow (carotid bifurcation)
- Plaque instability and rupture create thromboembolic debris and lead to neurological injury
- Plaque ulceration and thrombosis are associated with neurological symptoms, independent of degree of stenosis
During periods prone to ischaemia, collateral flow is critical for cerebral blood flow compensation and a major determinant of the severity of the ischaemic insult
Other factors include: plaque morphology, duration of hypoperfusion, characteristics of the embolus, and cerebral vasoreactivity.
The most common lesion found in patients with extracranial cerebrovascular disease is an atherosclerotic plaque in the carotid bifurcation. This produces symptoms by reducing blood flow or by releasing embolic material.
Carotid atherosclerosis and coronary atherosclerosis has distinct differences. Plaque ulceration, with embolisation of large amounts of necrotic core, is a common feature of carotid atherosclerosis.
Another mechanism for infarction with carotid stenosis is a sudden drop in systemic blood pressure leading to ACA-MCA watershed territory stroke
Classification
Based on symptomatic status
- Symptomatic: associated with focal neurological symptoms such as stroke, TIA, or amaurosis fugax in the last 6 months
- Asymptomatic: not associated with neurological symptoms in the last 6 months
Based on degree of stenosis:
- Mild (<50% diameter reduction)
- Moderate (50% to 69% diameter reduction)
- Severe (70% to 99% diameter reduction)
- Near occlusion (very tight and long stenosis from carotid bifurcation to the base of the skull in the range >95% with collapse of internal carotid)
- Total occlusion1
Clinical manifestations
- Asymptomatic
- TIA
- Stroke
Although carotid artery stenosis is one of the main causes of cerebrovascular disease, the aortic arch should always be assessed as this too is a site for atherosclerosis.
Anterior cerebral stroke:
- Contralateral weakness and sensory loss in lower limb
- Abulia (lack of motivation for action)
- Akinetic mutism (lack of movement and speech)
Middle cerebral stroke:
- Contralateral weakness and sensory loss of face and upper limb
- Ipsilateral gaze deviation
- Broca’s (expressive) aphasia
- Wernicke’s (receptive) aphasia
- Contralateral homonymous hemianopia
- Apraxia (inability to perform movements despite having desire and physical ability to do so)
- Neglect
ACA-MCA watershed stroke:
- “Man-in-the-barrel” syndrome (weakness in shoulders and hips bilaterally)
Ophthalmic artery:
- Amaurosis fugax (sudden and temporary loss of vision)
Examination
- Bruits over carotid arteries (best heard with the bell)
- Neurological and Cardiac exam
- Fundoscopy: cholesterol emboli
Absence of bruit does not always mean absence of disease as complete occlusions can be silent.
Differential diagnosis
- Arteriosclerotic disease (most common)
- Non-arteriosclerotic
- Fibromuscular dysplasia
- Dissection
- Vasospasm
- Aneurysm
- Arterio-venous fistula
- Vasculitides (Takayasu’s or Giant cell)
- Carotid body tumour
- Migraine with aura
Imaging:
- CT angiography (gold standard)
- MR angiography
- Carotid Duplex Ultrasound
- Digital Subtraction Angiography (for procedural planning)2
Treatment
Medical management
- Lifestyle modification
- Antiplatelets
- Statins
- Blood Pressure control
- Glucose control
Surgical management
Indications:
- Asymptomatic stenosis >70% (provided surgical risk is <2% and life expectancy >5 years)
- Symptomatic stenosis >50%
- High risk of stroke
Surgical options:
- Carotid endarterectomy
- Carotid artery stenting (when surgery is high risk)
Carotid endarterectomy is a procedure where the carotid artery is exposed surgically and temporarily clamped, the atherosclerotic material is shelled out, restoring cerebral blood flow and reducing the risk of cerebral ischaemia.
If artery is 100% occluded, do not operate – no benefit due to cerebral infarction already being complete and there is risk of embolus. Manage medically and operate on the other side to maximise perfusion.
Complications and Prognosis
Complications of stenosis
- Ischaemic stroke and all that comes with it
- Depression
Complications of endarterectomy and artery stenting
- Postoperative cerebral haemorrhage
- Cranial nerve injury
- Haematomas
- Stroke
- Myocardial infarction
- Restenosis
- Hyperperfusion syndrome – sudden increase in blood flow causing headaches, seizures and intracerebral haemorrhage
- Prognosis depends on degree of stenosis
References
- Lal BK, Bulbulia R. Carotid artery stenosis. In: BMJ Best Practice [Internet]. 2024 [cited 2025 Nov 19]. Available from: BMJ Best Practice
- Cucchiara BL. Evaluation of carotid artery stenosis. In: Kasner SE, Eidt JF, Mills JL, editor. UpToDate [Internet]. [updated 2024 Jan 04; cited 2025 Nov 19]. Available from: UpToDate
- Paraskevas KI, Mikhailidis DP, Ringleb PA, Brown MM, Dardik A, Poredos P, et al. An international, multispecialty, expert-based Delphi Consensus document on controversial issues in the management of patients with asymptomatic and symptomatic carotid stenosis. Journal of Vascular Surgery. 2024;79(2):420-35.e1. https://doi.org/10.1016/j.jvs.2023.09.031




Members only discussions coming soon…