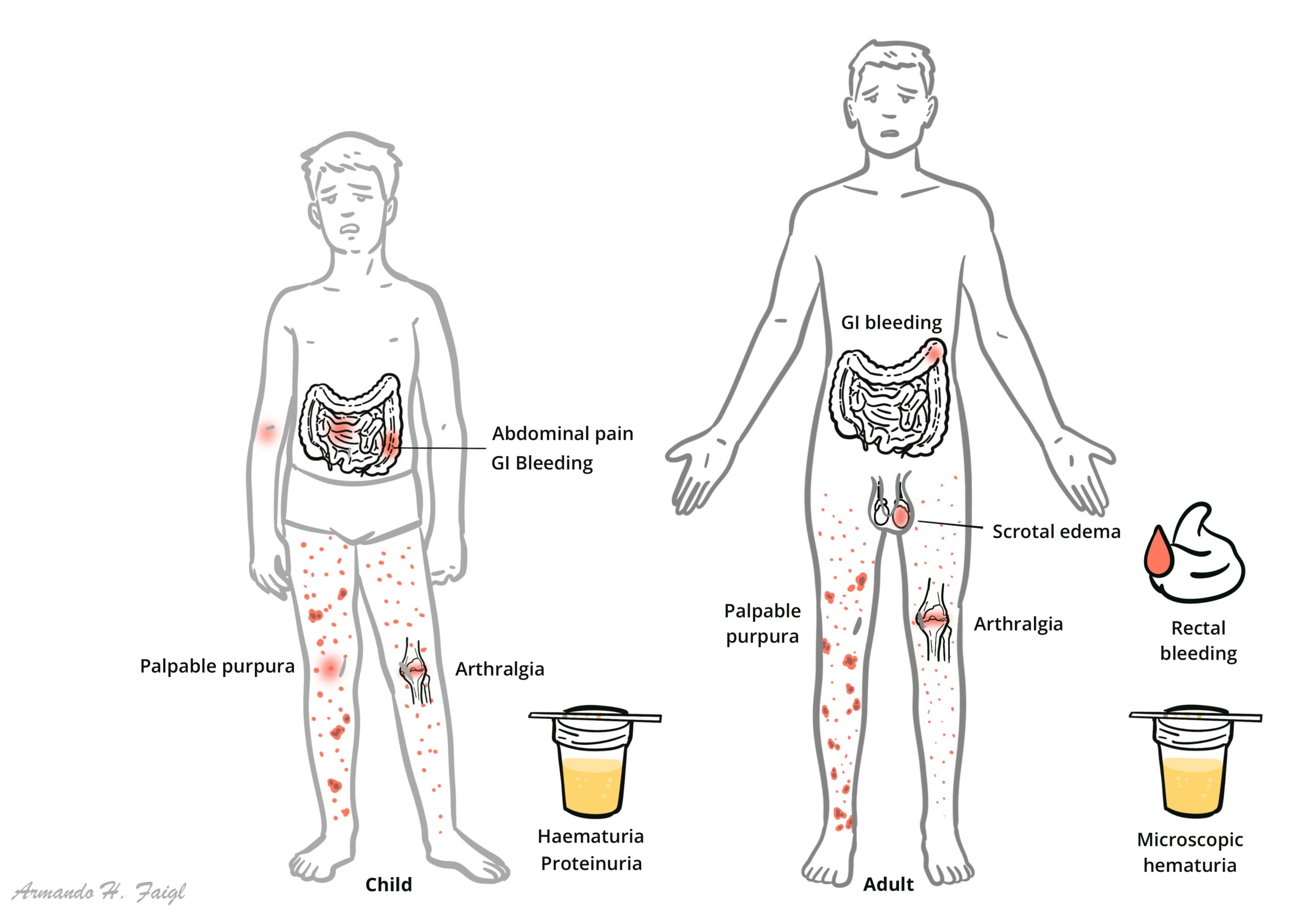
Henoch–Schönlein purpura (HSP), now termed IgA vasculitis, is the most common systemic vasculitis in children, characterised by IgA1-dominant immune complex deposition in small vessels, particularly affecting the skin, joints, gastrointestinal tract, and kidneys. It predominantly occurs in children aged 3–10 years, with a slight male predominance, and often follows an upper respiratory tract infection. The incidence is approximately 10–30 per 100,000 children per year. The disease is usually self-limiting but can have significant morbidity when renal involvement occurs.
Definition
IgA vasculitis:Small-vessel vasculitis with IgA-dominant immune complex deposition. Palpable purpura: Non-blanching, raised skin lesions due to vascular inflammation. IgA nephritis (IgAVN): Renal involvement characterised by IgA deposition in glomeruli. Leukocytoclastic vasculitis: Neutrophil-mediated small-vessel inflammation.
HSP = IgA-mediated small vessel vasculitis in children.
Anatomy and Physiology
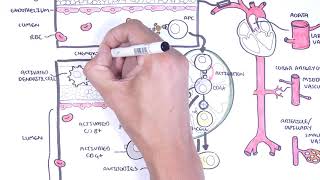
Small vessels: Capillaries, venules, arterioles—sites of immune complex deposition
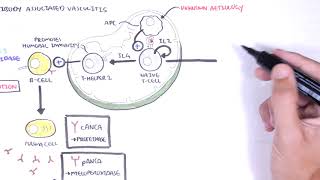
IgA function: Mucosal immunity; produced in response to infections
Complement system: Alternative and lectin pathways activated by immune complexes


















Discussion