

Post Traumatic Stress Disorder
Traumatic and Stress Related Disorders
- Post traumatic stress disorder
- Acute stress Disrorder
- Adjustment Disorder
This will mainly focus on PTSD
Overview
The identification of Post traumatic stress disorder (PTSD) in a patient involves understanding the traumatic event and the patient characteristics. PTSD may develop following exposure to 1 or more traumatic events such as deliberate acts of interpersonal violence, severe accidents, disasters, or military action.
Definition
Post traumatic Stress Disorder (PTSD): A syndrome that develops after a person witnesses, experiences, or is confronted with a traumatic event. The person reacts with feelings of helplessness, fear, and horror, and has ongoing symptoms of reexperiencing, avoidance of reminders, and symptoms of increased arousal.
Acute Stress Disorder: A syndrome that develops shortly after an individual is exposed to a traumatic event. It is characterized by intense fear and feelings of helplessness, as well as a number of dissociative symptoms. Acute stress disorder is defined as occurring within the first 4 weeks after a traumatic event (resolves without progressing to PTSD)
Adjustment Disorder: Characterized by mood disturbances (anxiety, depression) in response to a difficult situation, but adjustment disorders do not present with the avoidance symptoms (avoiding talking about the incident) and/or reexperiencing of the traumatic event.
Epidemiology The lifetime risk of being exposed to a traumatic stressor is high (60.7% for men, 51.2% for women), but only an estimated 8% of exposed men and 20% of exposed women develop PTSD.
Clinical Manifestations
Patients with PTSD may present in primary care with physical symptoms that are difficult to explain.
Re-experiencing the traumatic event
- Frequently having upsetting thoughts or memories about the traumatic event.
- Recurrent nightmares.
- Acting or feeling as though the traumatic event is happening again (flashbacks)
- Distress when reminded of the traumatic event
Avoidance and emotional numbing
- Avoiding thoughts, feelings, or conversations about the trauma.
- Avoiding places or people that remind the traumatic event.
- Having difficulty remembering important aspects of the event.
- Loss of interest in activities.
- Feeling distant from others.
- Restricted range of emotions
- Pessimism, hopelessness
Hyper-arousal (hypervigilance)
- Difficulty falling or staying asleep.
- Irritability and anger
- Difficulty concentrating
- Hypervigilance and accentuated startle response
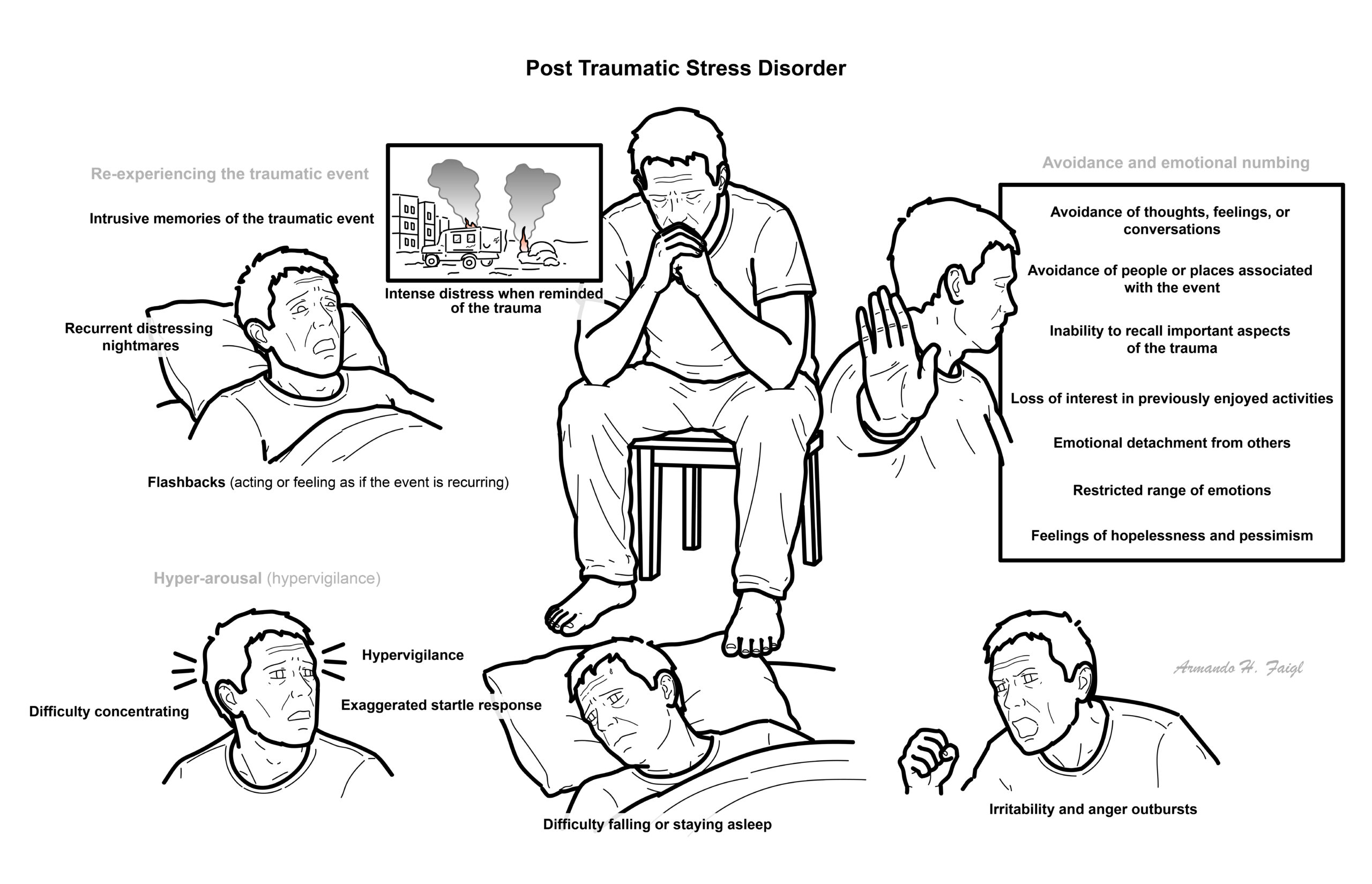
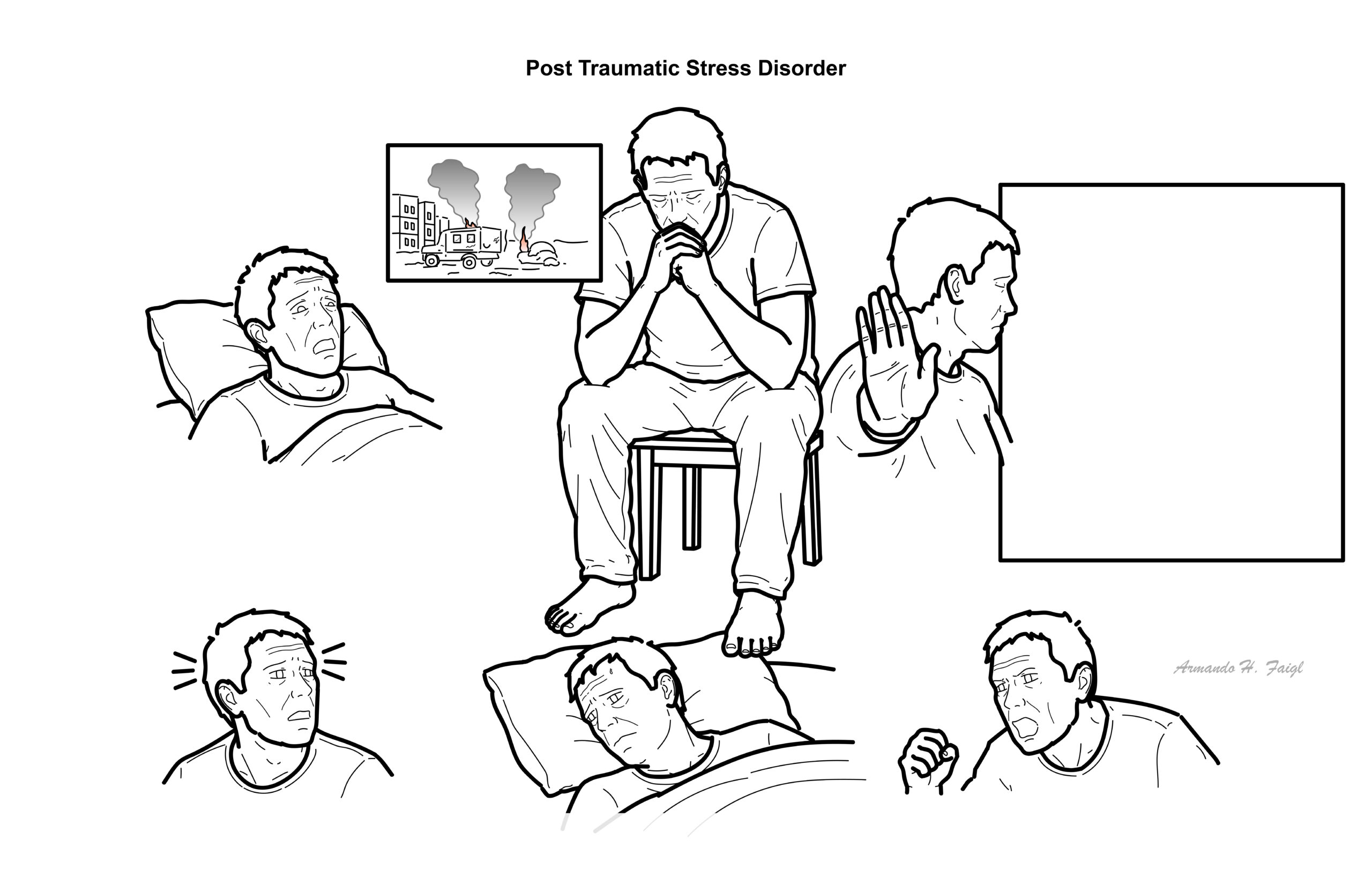
Triad of symptoms for PTSD: Re-experiencing, avoidance and hypervigilance.
Aetiology
PTSD can be due to indirect or direct forms of trauma
- Indirect
- Direct
Aetiology
- Exposure to war
- Threatened of actual physical violence
- Sexual violence
- Kidnapped
- Taken hostake
- Torcher
- Incarcerated as prisoner of war
- Terrorist attack
- Severe motor vehicle accident
- Traumatic surgical event – waking during surgery
- Witness of a natural
Individual reactions to traumatic events vary greatly and most people do not develop a mental disorder after exposure to trauma. PTSD should be considered in any patient exposed to a major traumatic event.
Diagnosis
Diagnosis (1-TRAUMAE)
- 1 month of symptoms (not necessary post trauma)
- Trauma exposure
- Re-experiences traumatic experience (Flashbacks, externally or internally triggers)
- Avoid triggers
- Unable to remember the trauma/ trust strangers
- Mood disturbance (Anhedonia)
- Arousal increased (increased stratal response)
- Exclude other medical conditions
Sensitive questioning is required to elicit symptoms of PTSD as patients may avoid volunteering their traumatic experience(s).
- Acute Stress Disorder
- Adjustment Disorder (The trigger is not that bad)
- Anxiety Disorder
- Major Depression
- Dissociative Disorder
- Personality Disorder
Post traumatic stress disorder is usually accompanied by a comorbid condition, such as major depression, another anxiety disorder, or substance dependence; this must be kept in mind when reviewing the differential diagnosis.
Patients can suffer injuries during traumatic events, and symptoms and sequelae of head injuries, particularly partial complex seizures can mimic symptoms of PTSD.
| CHARACTERISTICS OF TRAUMA AND STRESS RELATED DISORDERS | |||
| Acute Distress Disorder | Adjustment Disorder | PTSD | |
| Type of Stressors | Severe | Mild/Moderate | Severe |
| Time between stress and symptoms | Few days to maximum 4 weeks | Up to 3 months | Sometimes years |
| Duration of symptoms | Maximum one months | 6 months after end of stressors | >1month |
Pathophysiology
- Hyperstimulation of the Amygdala -> creates the fear response
- Underactive anterior cygulate gyrus -> usually mediates the fear response
- Decrease cortisol
- Increase ACTH, adrenaline and noradrenaline
Treatment
Trauma-focused psychotherapy and pharmacotherapy with selective serotonin reuptake inhibitors or serotonin–norepinephrine reuptake inhibitors are first-line treatment options for PTSD. Patient choice and availability of psychological therapy will influence the treatment given. Aim of treatment is to:
- Treat comorbid conditions, if any (e.g., depression, drug use)
- Dampen emotional arousal
- Deal with the meaning of the trauma
- Use exposure techniques to desensitise the patient from the disturbing memories
- Promote social skills
Non-pharmacological
- Clinical Debriefing Tutorial
- Trauma Focused Cognitive Behavioural therapy (CBT)
- Multiple session treatment
- Experience trauma through exposure therapy
- Confront the memory
- Eye movement desensitisation and reprocessing
- Cognitive Therapy
- Yoga
- Mindfulness
There is still debate whether early debriefing about traumatic event has better prognosis.
Pharmacological
- SSRI
- SNRI
Pharmacology
SSRI inhibits the reuptake of serotonin into the presynaptic neuron, increasing levels of serotonin the synaptic cleft. SSRI help with most PTSD symptoms, including intrusive thoughts and flashbacks, irritability and anger, problems concentrating, hyperarousal, chronic restlessness and anxiety, and depressed mood. Side effects: weight gain, drowsiness, depression, irritability, lethargy, fatigue.
Benzodiazepines should be avoided in the treatment of PTSD.
Complications & Prognosis
- Distress during therapy
- Anxiety
- Depression
- Psychosis
- Development of substance abuse
- Suicide
PTSD is associated with comorbidity.
Prognosis
- The average duration of symptoms, if treated, is 36 months, and the average duration of symptoms among those untreated is 64 months.
- Moreover, while almost 50% experience significant reduction in symptoms, more than one third of people never fully remit
References
Warner., CH, Warner., CM, Appenzeller., GN, & Hoge., CW (2013). Identifying and Managing Posttraumatic Stress Disorder. American Family Physician. 88(12). 827-834



Members only discussions coming soon…