Psoriatic arthritis (PsA) is a chronic, immune-mediated inflammatory arthritis associated with psoriasis, affecting up to 30% of patients with skin psoriasis. It commonly presents in adults aged 30–50 years, with equal gender distribution. The disease is highly variable, involving peripheral joints, axial skeleton, entheses, and skin/nails. Delay in diagnosis is common and can result in irreversible joint damage.
Definition
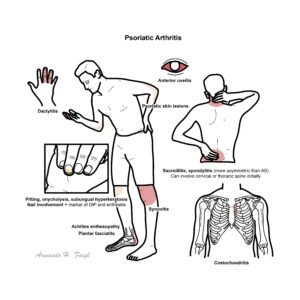
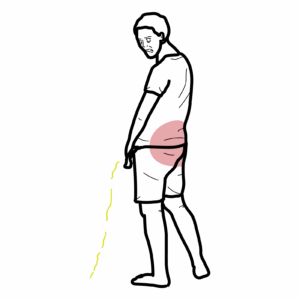
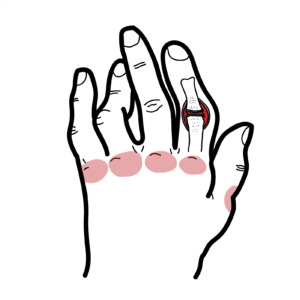
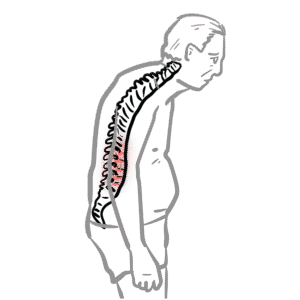
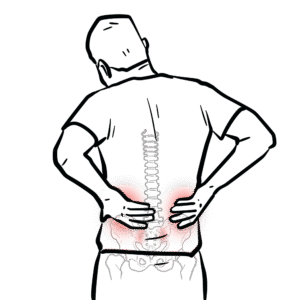
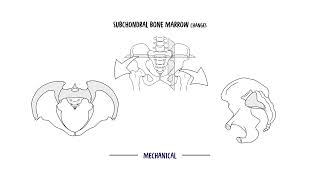
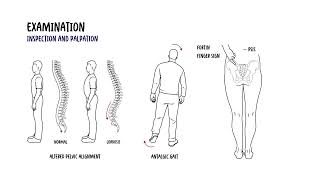
Psoriatic Arthritis (PsA): Seronegative spondyloarthropathy associated with psoriasis, affecting joints, entheses, and axial skeleton. Psoriasis Well-demarcated, erythematous plaques with silvery scale (often scalp, elbows, knees). Enthesitis: Inflammation at tendon or ligament insertion sites into bone. Dactylitis: Diffuse swelling of entire digits due to synovitis and tenosynovitis. Pencil-in-cup deformity: Classic radiographic change due to erosive and proliferative joint damage in PsA.
Mease PJ, Gladman DD, Papp KA, et al. Prevalence of rheumatologist-diagnosed psoriatic arthritis in patients with psoriasis in European/North American dermatology clinics. J Am Acad Dermatol. 2013;69(5):729–735.
Gossec L, Baraliakos X, Kerschbaumer A, et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheum Dis. 2020;79(6):700–712.
Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum. 2006;54(8):2665–2673.
Ogdie A, Weiss P. The epidemiology of psoriatic arthritis. Rheum Dis Clin North Am. 2015;41(4):545–568.













Discussion