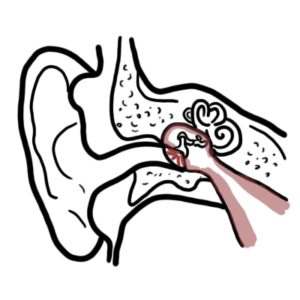
0:00 In this video, we're going to talk about acute otitis media. 0:09 Drived in the Greek word "ot", which means "ear", "itis", which means "inflamm 0:13 ation", 0:14 and from Latin media, which is something pertaining to the middle. 0:17 Acute otitis media is infection of the middle ear, and it is a very common 0:22 problem in children. 0:23 Now, the majority of children will be diagnosed with at least one episode of ot 0:27 itis media. 0:31 The ear plays a key role in hearing. The ear is divided into three parts, the 0:34 inner, middle and outer ear. 0:37 The basic physiology of the ear involves sound waves hitting and vibrating the 0:40 tympanic membrane. 0:42 The tympanic membrane moves the three small bones of the middle ear, the malle 0:46 us, incus, and stapes. 0:48 The movement of the stapes causes the fluid in the cochlea to vibrate. 0:54 The cochlea cells will translate this vibration, information into nerve 1:00 impulses, 1:01 and essentially send it to the brain where sound is perceived. 1:04 The eustachian tube is the connection between the middle ear and the nasal ph 1:08 arynx, or the nasal cavity. 1:11 The middle ear cleft is made up of the mastoid air cells posterior to the 1:20 middle ear cavity, 1:22 the eustachian tube, and the nasal pharynx. 1:25 The middle ear cleft can be thought of as a miniature lung. 1:31 These areas involve allow for ventilation and pressure equalization. 1:37 And any issues that occur within these areas can result in middle ear path 1:44 ologies. 1:45 The eustachian tube is a pretty important structure and serves many roles. 1:51 It permits equal abrasion of middle ear pressure with atmospheric pressure. 1:57 It's the primary defense mechanism of the middle ear. 2:05 It protects the middle ear from reflux of nasopharyngeal secretions through the 2:10 use of cilia, 2:11 propelling unwanted substances to the nasopharynx. 2:14 And thirdly, it drains secretions from the middle ear into the nasopharynx 2:21 because of the angle. 2:23 Acute otitis media mainly occurs in children and is a result of eustachian tube 2:28 dysfunction. 2:29 If the eustachian tube does not work, otitis media can develop. 2:33 For example, infection or a reaction in the middle ear cleft can result in ed 2:37 ema, swelling of the eustachian tube. 2:45 Similarly, adenoid hypertrophy from an infection can block eustachian tube 2:47 drainage and disrupt pressure equalization, 2:52 resulting in negative pressure in the middle ear. 2:56 Another cause of eustachian tube dysfunction is failure of some of the muscles 3:00 that connect or wrap around or pass through the eustachian tube. 3:05 This include failing of the tensor velli palatini and levatovelli palatini. 3:13 These muscles help in opening the eustachian tube, but are primarily used and 3:27 involved in swallowing and yawning. 3:32 Otitis media is more common in children, precisely because of the anatomical 3:36 differences of the eustachian tube between children and adults. 3:41 Unlike adults eustachian tube, the child's eustachian tube is more shorter, 3:49 more horizontally aligned, softer, and has a smaller passageway, and all this 4:02 allows for easier spreading of infection from the nasopharynx into the middle 4:02 ear. 4:02 The pathophysiology of acute otitis media follows a few stages. 4:11 One thing that people are often confused about is all the terminology used in 4:14 otitis media, such as otitis media with effusion, acute otitis media, suprative 4:20 otitis media, etc. 4:22 So hopefully understanding the pathophysiology and going step by step can help 4:26 clear this off. 4:28 So let's begin with a viral upper respiratory tract infection that has happened 4:32 for a few days. 4:34 This eventually causes congestion and swelling of the nasal mucosa, the nasoph 4:39 arynx, 4:40 and swelling of the eustachian tube. 4:42 Eustachian tube occlusion results in increased negative pressure in the middle 4:48 ear, and accumulation of middle ear secretions. 4:52 Secondary bacterial or viral infections can occur in this environment, which 4:58 will cause further separation and features of acute otitis media. 5:04 Remember, acute otitis media is a bacterial or a viral infection of the middle 5:10 ear. 5:11 However, in this closed environment, like what we discussed, certain bacteria 5:16 thrive. 5:17 The main causative bacterial agents in acute otitis media are streptococcus 5:23 pneumoniae, non-typable hemophilus influenza, and moraxella catarallis. 5:32 If the pressure becomes too great in the middle ear, because of fluid building 5:36 up, the tympanic membrane can perforate. 5:40 This is called suprative otitis media. 5:43 Suprative otitis media is characterized by ear discharge, termed oteria. 5:49 Suprative otitis media can become chronic, and thus is termed chronic suprative 5:54 otitis media. 5:57 Sometimes it resolves, and the perforated membrane heals, and returns to a new 6:02 baseline. 6:03 If the inflammation in the middle ear settles, there is resolution of symptoms 6:09 usually. 6:11 However, there is often residual fluid in the middle ear cavity. 6:16 Residual fluid in the middle ear cavity, after acute otitis media, is termed ot 6:22 itis media with effusion. 6:26 Otitis media with effusion is usually asymptomatic, and resolves by itself 6:31 after three months without doing anything. 6:33 Unfortunately, even though otitis media with effusion is asymptomatic, it is 6:39 still a potential environment for a reinfection, and this can thus cause 6:44 recurrent acute otitis media. 6:50 So let's look at a summary diagram of acute otitis media. Now, taking all the 6:56 pathophysiology into context, acute otitis media classically presents with at 7:00 algia, ear pain, pyrexia, fevers, hearing loss, and oteria, through the perfor 7:07 ation of the tympanic membrane. 7:09 Other symptoms in children include irritability, reduced appetite, upper 7:14 respiratory tract infections, and fatigue. 7:18 Otitis media with effusion is usually asymptomatic, as explained previously, 7:23 and typically follows an episode of acute otitis media. 7:27 Hearing loss is the other main complaint. Hearing loss occurs because the tymp 7:32 anic membrane and auditory ossicles are unable to move as effectively in an 7:37 environment full of fluid and inflammation. 7:42 Hence, in the presence of an infusion, there can be a conductive hearing loss 7:47 rather than a sensory neural hearing loss. 7:50 Diagnosis of acute otitis media and otitis media with effusion can be diagnosed 7:55 by direct visualization of the tympanic membrane with an otoscope or a pne 8:01 umatic otoscope. 8:04 In acute otitis media, the eardrum looks inflamed. Injections of the vessels of 8:10 the tympanic membrane to reddening with bulging of the eardrum is present. 8:15 Using a pneumatic otoscope, there is limited or absent mobility of the membrane 8:20 . Here is an image of an otoscope visualization of someone who has acute otitis 8:27 media. Note the bulging eardrum and blood vessels. 8:34 If there is perforation of the eardrum with discharge, this is termed supertive 8:38 otitis media. 8:40 Here is an image through an otoscope of someone with a supertive acute otitis 8:47 media. Note the discharge that is coming out. 8:51 Once diagnosis of acute otitis media is suspected, a period of observation is 8:56 recommended. Typically 24 to 48 hours is recommended. 9:02 These infections exist for high risk groups and persistent infections. The over 9:06 use of antibiotics may contribute to increasing antimicrobial resistance. Pain 9:10 and fever in acute otitis media should be controlled with paracetamol or ibupro 9:15 fen. 9:16 If symptoms do not improve with analgesia after 48 hours, then a course of 9:21 antibiotics is commenced. Typically, this is amoxicillin. 9:25 Decongestions and antihistamines are not beneficial in the treatment of acute 9:29 otitis media. 9:32 If acute otitis media resolves, it then really becomes otitis media with eff 9:36 usion, usually. 9:38 In otitis media with effusion, otoscopic findings include visualization of air 9:44 fluid levels with bulging and maybe decreased mobility of the tympanic membrane 9:49 . 9:50 There is no evidence of a red sore eardrum. Here is an image of otoscope 9:55 visualization of someone who has otitis media with effusion. 10:02 What's behind the tympanic membrane? 10:04 Recurrent otitis media or persistent otitis media with effusion may require 10:09 ventilation tubes, known as tympanostomy tubes. Especially the child has 10:14 features of hearing loss, developmental delays or learning difficulties. 10:22 It is also important to follow up on the child after episodes of an acute ot 10:28 itis media and to tell the parents to return if symptoms worsen, as this could 10:31 be signs of complications associated with acute otitis media. 10:36 Rare complications of acute otitis media can be divided into extracranial and 10:40 intracranial complications. 10:44 Most of the complications of acute otitis media is a result of direct extension 10:48 of the infection that pass to the mastoid air cells, which are situated behind 10:53 the posterior wall of the middle ear cavity. 10:57 Extension into the mastoid air cells causes mastoiditis. Other complications of 11:02 acute otitis media can include intracranial abscesses, including subjural abs 11:08 cess and subarachnoid abscess. 11:12 There can also be subperiosteal abscesses. Facial nerve palsy can be also a 11:17 complication, as well as labyrinthitis. 11:20 A more comprehensive video on the complications of acute otitis media and mast 11:25 oiditis will be available. 11:28 Adults can also present with acute otitis media and treatment is roughly the 11:32 same. 11:33 Remember, acute otitis media is a very common problem in children. 11:39 The majority of children will be diagnosed with at least one episode of otitis 11:42 media. 11:43 Management actually relies on a period of observation first, typically 24 to 48 11:49 hours before commencing antibiotics. 11:53 Thank you for watching.