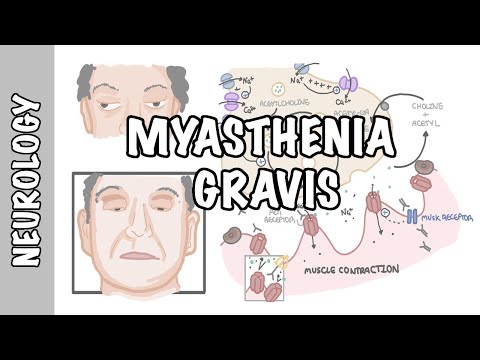
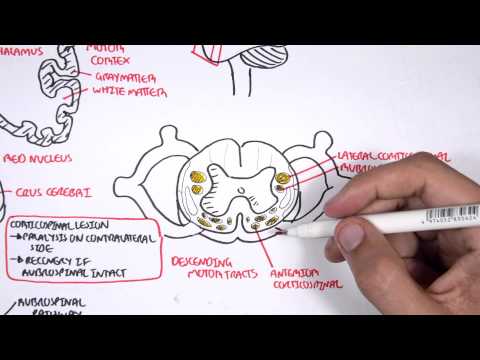
0:00 Lambert-Eton myosthenic syndrome is a neuromuscular junction disorder that was 0:10 first described 0:11 by Lambert, Eton, and Rook in the 1950s. 0:14 It is a disorder of voltage-gated calcium channels in the presynaptic motor 0:19 neurons, 0:19 the neurons that supply the skeletal muscles. 0:23 The voltage-gated calcium channels do not allow calcium influx, causing reduced 0:27 acetylcholine 0:28 release into the synaptic cleft, and thus reduced muscle contraction and 0:36 weakness. 0:38 Lambert-Eton myosthenic syndrome causes muscle weakness, which interestingly 0:42 improves with 0:43 activity, unlike the other neuromuscular junction disorder, myosthenic gravis, 0:48 which 0:48 manifests muscle fatigueability. 0:52 The more you use, the weaker the muscle gets. 0:56 Myosthenia can be divided into oculomyosthenia and generalized myosthenia. 1:02 Lambert-Eton syndrome is a perineoplastic syndrome because of its association 1:06 with small 1:07 cell lung cancer. 1:10 Perineoplastic syndrome can be described as an immunological phenomenon, but 1:14 really 1:15 are symptoms that occur at sites distant to where the tumor is. 1:25 The presynaptic neuron houses vesicles containing acetylcholine at its terminal 1:31 . 1:32 When an action potential travels along the neuron, the voltage-gated sodium 1:36 channels 1:36 open, allowing influx of sodium ions inside the cell. 1:41 This causes a positive electrical gradient, which then triggers voltage-gated 1:45 calcium 1:46 channels at the terminals to open up, allowing calcium ions to come inside the 1:52 cell. 1:53 Calcium ions trigger the vesicles to release acetylcholine in your transmitter, 1:58 into the 1:58 synaptic cleft, into the neuromuscular junction. 2:03 Acetylcholine binds to ligand-gated sodium channels, allowing sodium influx 2:09 into the 2:10 muscle, which eventually causes the muscle contraction. 2:15 And because of this, when you check reflexes normally, you have reflexes 2:19 present. 2:23 The causes of lambit-eaten myosynic syndrome can be either perineoplastic or 2:31 non-perineoplastic. 2:37 The thought is that the immune system mounts a response to voltage-gated 2:41 calcium channels 2:42 from cancer cells, creating antibodies against the voltage-gated calcium 2:48 channels, which 2:49 has a predilection to specific types of channels found in the neurons. 2:55 Non-perineoplastic causes are associated with autoimmune diseases such as 2:59 Graves' 3:00 disease and type 1 diabetes mellitus. 3:10 In lambit-eaten myosynic syndrome, these antibodies that are produced bind to 3:15 the voltage-gated 3:16 calcium channels are the terminal bulbs of motor neurons. 3:20 They are found to bind to the P-Q-type voltage-gated calcium channels, thus, 3:26 really preventing 3:27 calcium influx and then, subsequently, the release of acetylcholine into the 3:33 synaptic 3:33 cleft. 3:35 Because you have no acetylcholine, as a result, there is no muscle contraction. 3:39 You will have absent reflexes. 3:45 Current-eaten myosynic syndrome presents with proximal muscle weakness, mainly 3:49 the lower 3:49 limbs, absent reflexes, ptosis, autonomic disorders, including a dry mouth, 3:58 sluggish 3:59 pupils, and erectile dysfunction. 4:05 One of the hallmarks of lambit-eaten myosynic syndrome is post-exercise fac 4:12 ilitation. 4:13 This is essentially when one performs repetitive activities or repetitive 4:18 movements, instead 4:19 of fatigability, it forces depolarization and the release of acetylcholine into 4:24 the 4:25 synaptic cleft. 4:28 This post-exercise facilitation causes temporary improvement, which is the 4:33 hallmark of lambit-eaten 4:34 myosynic syndrome. 4:39 And so investigations to order for someone suspected of lambit-eaten syndrome 4:44 include 4:45 nerve conduction studies. 4:47 Here you will find reduced amplitude, with increased in amplitude on repetitive 4:53 stimulation. 4:54 So on repetitive movement, it actually gets better. 4:58 You can also check for voltage-gated calcium channel antibodies, and it's 5:03 important to 5:03 evaluate for malignancy, so for example by performing SCT chest. 5:15 Treatment involves treating the underlying malignancy, if found. 5:19 For mild symptoms, it's important just to monitor, however for moderate to 5:22 severe symptoms, 5:24 things such as amifambridine, a potassium channel blocker, can be used. 5:30 Normally, there are potassium efflux pumps, which causes repolarization, and so 5:36 inhibiting 5:36 these channels means you have depolarization, and so more acetylcholine can be 5:43 released into 5:44 the synaptic cleft, and then muscle contraction. 5:49 Other medications that can be used include guanidine and pyrostigmine, which is 5:55 an acetylcholinesterase 5:57 inhibitor, acetylcholinesterase is an enzyme which breaks down acetylcholine in 6:03 the synaptic 6:04 cleft. 6:08 By blocking this enzyme with pyrostigmine, you prolong the effects of acetylch 6:13 oline, which 6:13 then binds onto the ligand-gated sodium channels, allowing sodium influx and 6:19 muscle contraction. 6:21 Thank you for watching this video, I hope you enjoyed it. 6:23 We talked about the different causes of Lambert-Eton myocenic syndrome, paran 6:27 ioplastic and non-paranioplastic, 6:29 as well as the clinical features, including weakness, which interestingly 6:33 improves with 6:34 movement, as well as investigations, including the CT chest and the antibodies. 6:41 Thank you for watching, I hope you enjoyed this video. 6:53 Thanks for watching!