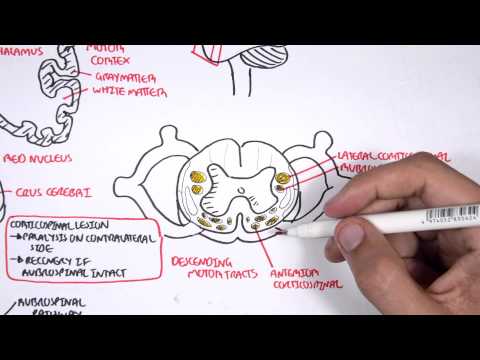
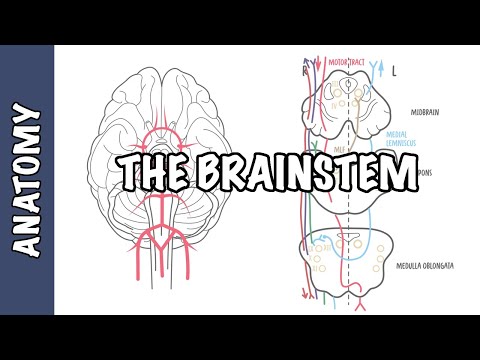
0:00 In this video, we're going to talk about medullary lesions, so lesions that 0:09 occur in 0:09 the medulla oblongata and how they present clinically. 0:14 At this point, before discussing these clinical cases, it is important to 0:18 introduce the rules 0:19 of the fours, of the brainstem. 0:27 So the rules of four, as the name suggests, there are four rules. 0:33 And within each of these rules, it is all related to four, basically. 0:38 So the first rule of the rules of four is that there are four structures in the 0:45 midline 0:46 of the brainstem, beginning with M. And these are the motor pathways or the 0:53 cortical spinal 0:54 tract, which passes the midline, the medial lemoniscus, the medial longitudinal 1:00 fasciculus 1:01 and the pathway, as well as the motor nuclei and cranial nerves, which are also 1:09 located 1:10 the nuclei in the midline. 1:16 The second rule of the rule of fours is that there are four structures to the 1:23 side, or lateral, 1:25 beginning with S, so S for sides. 1:29 And these structures are the spinocerebella pathway, the spinothalamic pathway, 1:36 the sensory 1:37 nuclei of the fifth cranial nerve are located laterally, as well as the 1:43 sympathetic pathway. 1:45 The third rule of the rule of fours is that there are four cranial nerves in 1:54 the medulla, 1:56 which is the bottom part of the brainstem. 1:58 There are four cranial nerves in the pons and four cranial nerves above the p 2:03 ons, two 2:04 in the midbrain and two above. 2:08 So again, above the pons there are cranial nerves one, two, three, and four. 2:14 Cranial nerves three and cranial nerves four are within the midbrain. 2:19 In the pons there are cranial nerves five, six, seven, and eight. 2:24 And in the medulla there are cranial nerves nine, ten, eleven, twelve. 2:30 The last rule, the fourth rule of the rule of fours is that the four cranial 2:37 nerve nuclei 2:39 that are in the midline can be easily remembered by being divisible or that can 2:46 divide equally 2:48 into twelve, except one and two. 2:51 So the four cranial nerves I'm talking about that are in the midline and divide 2:56 equally 2:56 into twelve include cranial nerves three, cranial nerves four, six, and twelve. 3:05 Cranial nerves five, seven, nine, and eleven are in the lateral aspect of the 3:10 brainstem. 3:11 What makes this even more interesting is that the cranial nerves at the midline 3:18 , so three, 3:19 four, six, and twelve, are all motor nerves. 3:29 Now to try to understand the rules of four for the brainstem, let's work 3:35 through some 3:35 examples focusing on lesions that occur in the medulla oblongata. 3:42 The first case is an elderly woman that presents with sudden, right-sided horn 3:48 et syndrome, 3:48 erotosis, meiosis, and anhydrosis on the right side, with left-sided loss of 3:56 pain and temperature 3:58 sensation below the neck in the arms and the legs, with associated difficulty 4:04 swallowing. 4:05 But the elderly woman has loss of sensation to the right side of the face. 4:12 The patient also complains of vertigo, nausea, and vomiting. 4:16 There is no limb weakness noted by the patient. 4:22 The signs and symptoms are caused by an injury to the lateral aspect of the med 4:27 ulla, usually 4:29 as a result of an infarction of the posterior inferior cerebellar archery. 4:36 This causes what is called Wallenberg syndrome, also known as lateral medullary 4:41 syndrome. 4:42 But in this case, the lesion is on the lateral aspect of the medulla, and in 4:48 this case, the 4:49 lesion is on the right lateral aspect of the medulla. 5:00 And so looking at it in a bit more detail, when you have the lesion on the 5:06 lateral aspect, 5:07 on the right side, you can see the structures that are involved. 5:12 Firstly, you have involvement of the sympathetic fibers, on the right side, 5:18 which will result 5:19 in ipsilateral hornet syndrome, so hornet syndrome on the same side. 5:29 Involvement of the lateral spinothalamic tract results in contral lateral loss 5:34 of pain and 5:35 temperature sensation below the neck. 5:40 Involvement of the inferior cerebellar peduncle will result in the ataxia. 5:46 The difficulty swallowing is due to involvement of the vagus and glossopharynge 5:51 al nerve at 5:51 the medulla oblamgata level. 5:55 Now please note that this patient has no limb weakness, and this is because the 6:00 motor fibers, 6:01 the corticospinal tract is in the medial aspect of the medulla, not the lateral 6:09 . 6:09 And also note that this patient has no loss of basic touch and vibration below 6:16 the neck, 6:17 and this is because the medial lemaniscal tract runs in the medial aspect of 6:24 the medulla. 6:26 But to make this a bit more complicated, some of the cranial nerve nuclei from 6:31 the pons, 6:32 which is above, naturally extends down to the medulla level. 6:37 So involvement of the inferior vestibular nucleus will cause vertigo, nausea 6:45 and vomiting. 6:46 Involvement of the spinal aspect of the trigeminal nerve causes ipsilateral 6:51 loss of sensation 6:52 to the face, so loss of sensation to the right side of the face. 6:58 The trigeminal nerve, if you recall, is important for sensation of the face. 7:10 The second case to look at is of an elderly man who presents with sudden left- 7:15 sided weakness 7:17 of his body, and on examination you also notice that this person has tongue 7:23 deviation to the 7:24 right side, and you find that there is a decrease in his vibration and touch 7:29 sensation on the 7:30 left side as well. 7:34 Now these signs and symptoms are caused by an injury to the medial aspect of 7:39 the medulla, 7:40 which affects also the hypoglossal nerve and nuclei, cranial nerve, you know, 7:46 12. 7:47 This syndrome is called diorine syndrome, or medial medullary syndrome, and it 7:55 is caused 7:56 by an occlusion of the small perforating branches, the blood vessels 8:02 originating from 8:02 the vertebral or proximal basilar arteries, or occlusion of the anterior spinal 8:08 artery 8:08 as well. 8:10 Now in this case, the lesion is on the right side, the right medial aspect of 8:22 the medulla. 8:24 Now when you have a lesion here, or an infact here, these structures are 8:30 involved, so involvement 8:32 of the right motor pyramidal tract, which results in your contralateral 8:38 opposite side, paralysis, 8:41 weakness of the upper and lower limbs of the body, so on the left side, you 8:45 will have 8:45 involvement of the hypoglossal nerve fibers on the right side, which results in 8:50 tongue 8:50 deviation to the affected side, so to the right side. 8:57 You'll have involvement of the right medial lemoniscal tract, which results in 9:03 contralateral 9:04 decrease in sensation for vibration and fine touch. 9:09 Now I hope all those two cases make sense, but it's good to appreciate the 9:16 rules of 9:17 four of the brainstem and how you can apply it to the clinical picture. 9:26 So in summary, we discussed the rules of four and the clinical relevant cases 9:30 of Wallenberg 9:31 syndrome, also known as lateral medullary syndrome, and dejureme syndrome, also 9:37 known 9:37 as medial medullary syndrome. 9:39 Thank you for watching. 9:47 [BLANK_AUDIO]