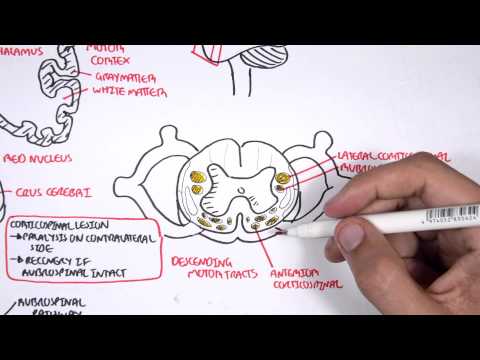
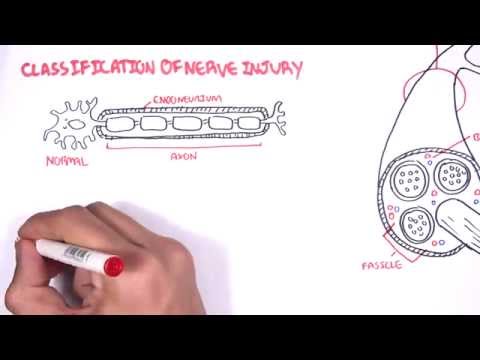
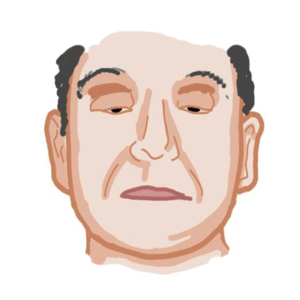
0:00 Hello, in this video, we're going to look at the clinical anatomy of the spinal 0:11 cord. 0:11 Now, the spinal cord is part of your central nervous system. 0:15 The spinal cord is the continuation of the brain and the brain stem. 0:19 The spinal cord's termination is called the conosmodularis, which ends at about 0:24 the L2 0:25 vertebral level. 0:26 On this point on, you have continuing nerve fibers extending down, known as a c 0:31 ote quanae 0:31 or the horse's tail. 0:34 The spinal cord is protected and goes through the spinal canal, which is 0:38 basically made 0:38 up of the vertebrae, the bones. 0:42 The vertebrae is divided into sections. 0:44 You have seven cervical vertebraes. 0:46 You have 12 thoracic, five lumber. 0:48 You have the sacrum, and then you have the coccyx. 0:51 Like the vertebrae, the spinal cord is also divided into sections. 0:54 You have the cervical, thoracic, lumber, sacral, and coccyx sections. 0:59 Each spinal cord section have or segments have nerves coming in and out of it. 1:05 These are known as the spinal nerves. 1:07 The spinal nerves exits from their corresponding vertebral level. 1:12 Let's take a look at the cervical spinal cord, which is unique because it has 1:17 eight pairs 1:18 of spinal nerves. 1:20 The cervical spinal cord is drawn in green here. 1:24 It's unique because the cervical spinal nerve exits over their corresponding 1:29 vertebral level. 1:31 For example, the C1 spinal nerve, the cervical 1 spinal nerve goes over the 1:37 cervical 1 vertebral 1:39 level, vertebral body, and so on, until you have cervical 8, C8, which exits 1:46 over the thoracic 1:48 1 vertebra. 1:51 And this is because there is no C8 vertebra, obviously. 1:57 The thoracic spinal cord is here in blue, and it has 12 pairs of thoracic 2:03 spinal nerves. 2:04 The thoracic spinal nerve exits below their corresponding vertebrae. 2:10 T1 exits below the T1 vertebra, T12 spinal cord exits below the T12 vertebra. 2:21 The lumbar spinal cord here in purple has five pairs of lumbar spinal nerves, 2:26 exiting 2:27 again below their vertebral sections. 2:30 Example, you have the L1 spinal nerve exiting below the L1 vertebra. 2:36 The sacral spinal cord have five pairs of spinal nerves, which exits through 2:41 the sacral 2:42 holes. 2:43 Finally, you have the cocisigial nerve, which exits below the coccyx. 2:58 Looking closely at the spinal cord now and the vertebrae, in more detail, we're 3:02 looking 3:02 at the thoracic vertebrae as an example. 3:08 The spinal cord goes through the spinal canal of the vertebra. 3:11 The vertebral disc sits in between the vertebrae. 3:17 The spinal cord have thoracic spinal nerves coming out, here represented in 3:25 blue. 3:27 The spinal cord have the anterior spinal artery and two posterior spinal 3:31 arteries supplying 3:32 it. 3:38 Let's look at a superior view of the thoracic spinal cord and vertebrae now. 3:46 Interior to the vertebral body is the thoracic aorta. 3:49 The thoracic aorta have posterior artery branches called the posterior inter 3:55 costal arteries, 3:56 which will supply the ribs. 3:58 The posterior intercostal arteries branch to form the posterior spinal artery 4:04 and also 4:04 gives rise to the anterior spinal artery in the thoracic section of the spinal 4:17 cord. 4:18 Let's now focus on the spinal cord in more detail. 4:25 Let's take a cross section of the thoracic spinal cord. 4:29 The spinal cord has a central butterfly looking structure. 4:32 The dorsal root at the back and the ventral root in the front will form the 4:38 spinal nerve. 4:40 In this case, it would be the thoracic spinal nerve. 4:44 The spinal nerve then a branch and can form the dorsal ramus and the ventral 4:49 ramus, which 4:50 essentially will supply and innervate different parts of the body. 4:57 Let's now take a cross section of the cervical spinal cord. 5:01 The butterfly looking structure in the center of the spinal cord is the gray 5:05 matter of the 5:06 spinal cord. 5:07 The gray matter is where synapses between neurons occur. 5:12 Here we can find the dendrites and the terminal axons of neurons. 5:18 This is where synapses occur. 5:20 The white matter surrounding the gray matter is where neurons travel through 5:27 along the 5:28 spinal cord. 5:29 It therefore contains a neuron's axons. 5:33 As we learned, the ventral root is found in the anterior aspect of the spinal 5:39 cord. 5:40 The ventral root of the spinal cord carries motor neurons out from the spinal 5:45 cord. 5:46 The dorsal root of the spinal cord carries sensory information into the spinal 5:50 cord and 5:50 so here we also find the spinal sensory ganglion where the sensory neuron's 5:57 body is located. 5:59 The dorsal and ventral root will form the spinal nerve. 6:03 This in this case is a cervical spinal nerve. 6:08 Let's take a look at a cross section of the lumbus spinal cord now. 6:13 The lumbus spinal cord typically has a large gray matter. 6:17 The dorsal root of the spinal cord carries sensory information. 6:25 For example, information from the skin which contains sensory nerve fibers. 6:31 When touch, pain is felt, these sensory fibers will carry information to a 6:35 particular spinal 6:36 cord level. 6:38 The sensory neuron's body is at the dorsal root ganglion. 6:44 The sensory neuron will travel to the posterior horn of the spinal cord. 6:51 The anterior horn of the spinal cord is where the lower motor neurons arise and 6:55 they will 6:56 exit the spinal cord through the ventral root and target an infected organ, for 7:03 example, 7:03 the muscle. 7:08 To complete this section here, we have the sacral spinal cord and the coccigio 7:13 le spinal 7:13 cord cross section. 7:18 Remember the spinal cord ends at about the L1, L2 vertebral level and this is 7:23 termed the 7:24 cognizumidolaris. 7:26 Continuing bundle of fibers from here is a coda equana. 7:35 Let's talk about dermatomes. 7:38 Your skin is innervated by sensory nerve fibers. 7:46 Dermatomes are sensory nerve fibers that innervate a segment of skin and is 7:51 associated with a 7:52 single spinal cord level. 7:54 So for example, here is a human body with a dermatomal distribution drawn out. 8:10 This area in green here is innervated by spinal nerve fibers from the cervical 8:18 spinal 8:18 cord. 8:22 The dermatome drawn in green here correlates with different sections of the 8:27 cervical spinal 8:28 cord. 8:31 This area has sensory nerve fibers which will bring information to the C6 8:37 spinal cord level. 8:47 Here is C2, C3, C4, C5, C6, C7, and C8. 8:52 We have eight cervical spinal nerves. 9:01 These segments are the dermatomal distribution of the thoracic spinal cord in 9:09 blue. 9:10 T1 spinal cord and so on, T10 is easy to remember because it is along the umbil 9:17 ical level. 9:19 The segments of skin is innervated by the lumbar nerve sensory fibers. 9:26 For example, this area in particular on the knee is innervated by sensory nerve 9:31 fibers 9:31 which will bring information to the L4 spinal cord level. 9:42 The skin segments in orange is a dermatological distribution of the sacral 9:46 spinal cord levels. 9:48 These include the genitals, part of the foot, but mainly the posterior aspect 9:51 of the lower 9:52 limb. 9:56 Here is the back of the left leg. 9:58 As you can see it is innervated by the sacral spinal nerves. 10:08 Important to know that S3, S4, S5 dermatome distribution is important in 10:14 assessing sensation 10:16 of the anus. 10:18 This area is tested for sensation to see if there is any signs of spinal cord 10:26 injuries. 10:27 To complete this image, let's talk about the face. 10:32 The side of the face, as you can see, is innervated by C2, C3, C4, dermatomal 10:40 distribution. 10:42 The front of the face is not innervated by the cervical spinal nerves, but 10:47 rather they 10:47 are innervated by the trigeminal nerve, which is cranial nerve number 5. 10:53 After learning a bit about dermatomes and sensory nerve fibers, we can now 10:57 discuss some 10:57 clinical anatomy focusing on the herpes zoster infection, also known as shing 11:02 les. 11:02 Shingles is a common infection. 11:04 It's the reactivation of the varicellar zoster virus, which is the chicken pox 11:08 virus, in the 11:09 sensory dorsal root or cranial nerve ganglion. 11:12 It manifests in the elderly usually and is characterized by a vesicular rash 11:18 along a dermatomal 11:19 distribution. 11:21 Shingles classically has a pro-drome phase characterized by pain, burns, and 11:27 sharp sensation 11:28 like itching and tingling as well. 11:31 This is followed by an eruption of a rash, usually unilateral vesicular rash, 11:37 which will 11:38 eventually ulcerate and crust over in 10 days. 11:42 Remember, it usually manifests along a specific dermatomal distribution, 11:47 unilateral on one 11:48 side. 11:50 To understand the pathophysiology briefly, let's look at the T7 spinal cord 11:55 level, which 11:56 innervates the T7 dermatome segment of the skin, which is basically the upper 12:04 abdomen. 12:05 Shingles is reactivation of the chicken pox virus. 12:09 What happens is that the chicken pox virus infects a child, characterized by a 12:14 vesicular 12:14 infectious, contagious rash all over the face and upper body. 12:20 The virus can obviously affect the T7 dermatome, and then it can invade the 12:27 area and travel 12:28 along the sensory nerve fiber and essentially rest, stay dormant in the dorsal 12:34 root ganglion. 12:36 Years later, when the child gets old, the chicken pox virus, also known as the 12:40 varicyloster 12:41 virus, can reactivate, maybe due to immunosuppression or whatnot. 12:45 But essentially, it will become the herpes zoster virus, which will travel back 12:50 up the 12:50 sensory nerve fiber and express itself along the T7 dermatomal distribution as 12:56 shingles. 12:57 Here is a photograph of a person who suffers from shingles, and you can see 13:10 that there 13:12 is a vesicular crusting rash along the trigeminal V1 dermatomal distribution. 13:23 Here is another example of a person's back, and you can see the rash, vesicular 13:29 rash is 13:30 unilateral and it affects the dermatomal distribution roughly T1 to T3 dermat 13:39 omal distribution, 13:40 the thoracic area. 13:42 Let's talk about the blood supply to the spinal cord, which we already briefly 13:50 mentioned. 13:51 The spinal cord receives two main blood supplies, the two posterior spinal 13:55 arteries and the anterior 13:57 spinal artery. 13:58 These arteries run along the spinal cord. 14:02 The posterior and anterior spinal arteries are branches of different arteries 14:07 depending 14:08 on the segment or the section of the spinal cord. 14:12 For example, the upper spinal cord posterior and anterior spinal arteries arise 14:18 from the 14:19 vertebral artery, a branch of the subclavian artery. 14:24 The spinal arteries also arise from the branch of the subclavian artery called 14:32 the ascending 14:33 cervical artery. 14:36 On the thoracic level, the thoracic aorta have branches called the posterior 14:41 intercostal 14:42 arteries, which we talked about. 14:44 That gives rise to the posterior and anterior spinal cord arteries. 14:49 The lower spinal cord arteries are branches of the lumbar artery, which is a 14:54 branch of 14:54 the abdominal aorta, as well as the lateral sacral artery, a branch of the 15:01 internal iliac 15:02 artery. 15:06 The artery of, I hope I pronounce this right, at am quits is an important 15:13 artery. 15:14 It is the primary supply to the lower two thirds of the spinal cord. 15:19 Essentially, if there's occlusion of the artery of at am quits due to schema 15:26 hypertension 15:26 or whatever, it can cause a person to be paraplegic. 15:32 Because again, it supplies, it's the main supply to the lower two thirds of the 15:35 spinal 15:36 cord. 15:41 Next let's talk about the meninges, the layers that surround the spinal cord 15:46 and protect 15:46 it. 15:51 Meninges comprise of three layers of protective tissue. 15:54 Just like you have meninges of the brain, this continues to form the meninges 15:58 of the 15:59 spinal cord. 16:00 Here I am drawing the spinal cord and I will introduce the meningial layers one 16:06 at a time, 16:06 from the very inner one to the outer one. 16:10 And there are three meningial layers. 16:13 The pia matter is the inner meningial layer surrounding the spinal cord. 16:18 The second layer is the arachnoid membrane, which extends to the spinal nerve. 16:25 Between the pia matter and the arachnoid membrane is the arachnoid space. 16:31 The outermost meningial layer is the dura matter. 16:35 Between the dura matter and the arachnoid membrane is the sub-dural space. 16:42 The sub-dura matter is the epigural space. 16:46 Now within the arachnoid space, the sub-arachnoid space, you can find fluid 16:51 flowing through 16:52 it called the cerebrospinal fluid. 16:55 The cerebrospinal fluid also flows through the central canal at the middle of 17:00 the spinal 17:00 cord. 17:02 Cerebrospinal fluid, also known as CSF, provides the brain and spinal cord with 17:07 nutrients. 17:08 CSF is produced in the brain's ventricles. 17:14 Let's look at the side view of the spinal cord again and understand the mening 17:19 ial layers. 17:20 The spinal cord ends at the colonist medallaris and the extension of the nerve 17:25 fibers is the 17:26 cate quanet. 17:29 Then you have this thing called the phillum terminale, which is basically 17:34 connective tissue, 17:36 strand continuing on from the colonist medallaris and extends all the way to 17:44 basically the coccyx. 17:45 The phillum terminale is divided into the phillum terminale internus, which is 17:49 made up of continuation 17:52 of the pia matter, and then you have the phillum terminale externus, which is 17:58 made up of the 17:58 dura matter and the arachnoid membrane. 18:02 The phillum terminale externus ends at the coccyx. 18:07 The space after the colonist medallaris below L2 is a site where cerebrospinal 18:15 fluid can 18:16 be accessed. 18:19 This space is a subarachnoid space. 18:24 A lumbar puncture is a procedure of collecting cerebrospinal fluid from the 18:29 spinal canal. 18:31 This is a zoomed section of the lumbar region, L2, L3, L4 and the L5 vertebra. 18:38 The spinal cord ends again about the L2 vertebral level. 18:42 Then you have the continuing cate quanet, the horse's tail. 18:46 The pia matter ends and continues as the phillum terminale internus inferiorly. 18:53 The cate quanet is within the arachnoid space floating around. 18:59 The whole area is surrounded by the arachnoid membrane, and then you have the d 19:05 ura matter 19:05 after that. 19:09 The arachnoid membrane and dura matter, as we know, continue down and then 19:13 envelopes 19:14 to form the phillum terminale externus. 19:18 Above the dura matter is the epigural space. 19:23 Let us progress out, let us now look at the layers after the epigural space. 19:30 First, the vertebrae is supported by many ligaments. 19:35 Behind the spinal cord you have the ligament of phillum, intraspinous ligament, 19:41 then you 19:41 have the supraspinous ligament. 19:44 Surrounding the spinous process and the supraspinous ligament is the subcut 19:49 aneous tissue and then 19:50 you have the skin. 19:53 The goal of a lumbopunctur is to collect subraspinous fluid, which can be done 19:58 by sticking a needle 19:59 through the skin, subcutaneous tissue, supraspinatus ligament, intraspinous 20:06 spinal ligament, ligamentum 20:08 flavum, dura matter and the arachnoid membrane into the subarachnoid space 20:15 where the CSF, 20:15 the subraspinous fluid is present. 20:18 Once the needle is in the space, CSF fluid should drip out. 20:23 The needle is typically inserted between the L4, L5 vertebral level to make 20:28 sure it does 20:29 not hit the spinal cord. 20:32 A lumbopunctur is both diagnostic and therapeutic, therapeutic because it 20:36 allows intrathecal administration 20:38 of chemotherapy and antibiotics, for example. 20:42 It can help diagnose meningitis and multiple sclerosis. 20:48 Here is an image of a lumbopunctur being performed. 20:53 Note the needle in the patient's back. 20:55 Most likely it is inserted between the L4 and L5 or L3 and L4 vertebral level 21:01 and note 21:02 CSF dripping slowly out of the needle and being collected by a small tube. 21:08 Also note the sterile field which is important to prevent the introduction of 21:12 infection to 21:14 the spinal cord. 21:18 Clinical anatomy, obviously the spinal cord can be injured. 21:22 These are classically called spinal cord injuries or lesions or syndromes. 21:28 Spinal cord lesions have many causes including penetrating injuries, crush 21:32 injuries, gunshot 21:33 injuries, tumours, abscess, you name it. 21:37 Spinal cord lesions can be divided into a few classic types. 21:42 You have complete transection of the spinal cord, hemisection of the spinal 21:47 cord, central 21:48 spinal cord lesions, posterior spinal cord lesions and anterior spinal cord 21:54 lesions, all 21:55 of which present with differing sensory and motor deficits. 22:00 We won't talk about that in this video but there will be hopefully other videos 22:03 that 22:03 will go into more detail. 22:05 Thank you for watching this video. 22:06 I hope it helped. 22:07 I hope you enjoyed it. 22:08 Thanks for watching. 22:09 I hope you enjoyed it. 22:10 I hope you enjoyed it. 22:11 Thank you. 22:12 I hope you enjoyed it. 22:13 Thank you. 22:14 I hope you enjoyed it. 22:15 Thanks for watching. 22:16 I hope you enjoyed it. 22:17 I hope you enjoyed it.