

Hydroxyapatite Deposition Disease
Overview
Hydroxyapatite Deposition Disease (HADD) is a crystal-induced tendinopathy caused by the deposition of hydroxyapatite (HA) crystals, typically in periarticular soft tissues, especially tendons and bursae. The shoulder (supraspinatus tendon) is most commonly affected. It often presents between ages 30–60, more frequently in women. While often asymptomatic, it can cause acute pain and functional limitation during resorptive phases.
Definition
Hydroxyapatite (HA): A calcium phosphate crystal naturally found in bone but pathologically deposited in soft tissues.
HADD: Disease resulting from abnormal deposition of HA crystals in tendons or bursae, leading to pain and inflammation.
Calcific tendinitis: Clinical term describing symptomatic HADD, often in the shoulder.
Periarticular: Refers to structures surrounding a joint (e.g. tendons, bursae).
Anatomy and Physiology
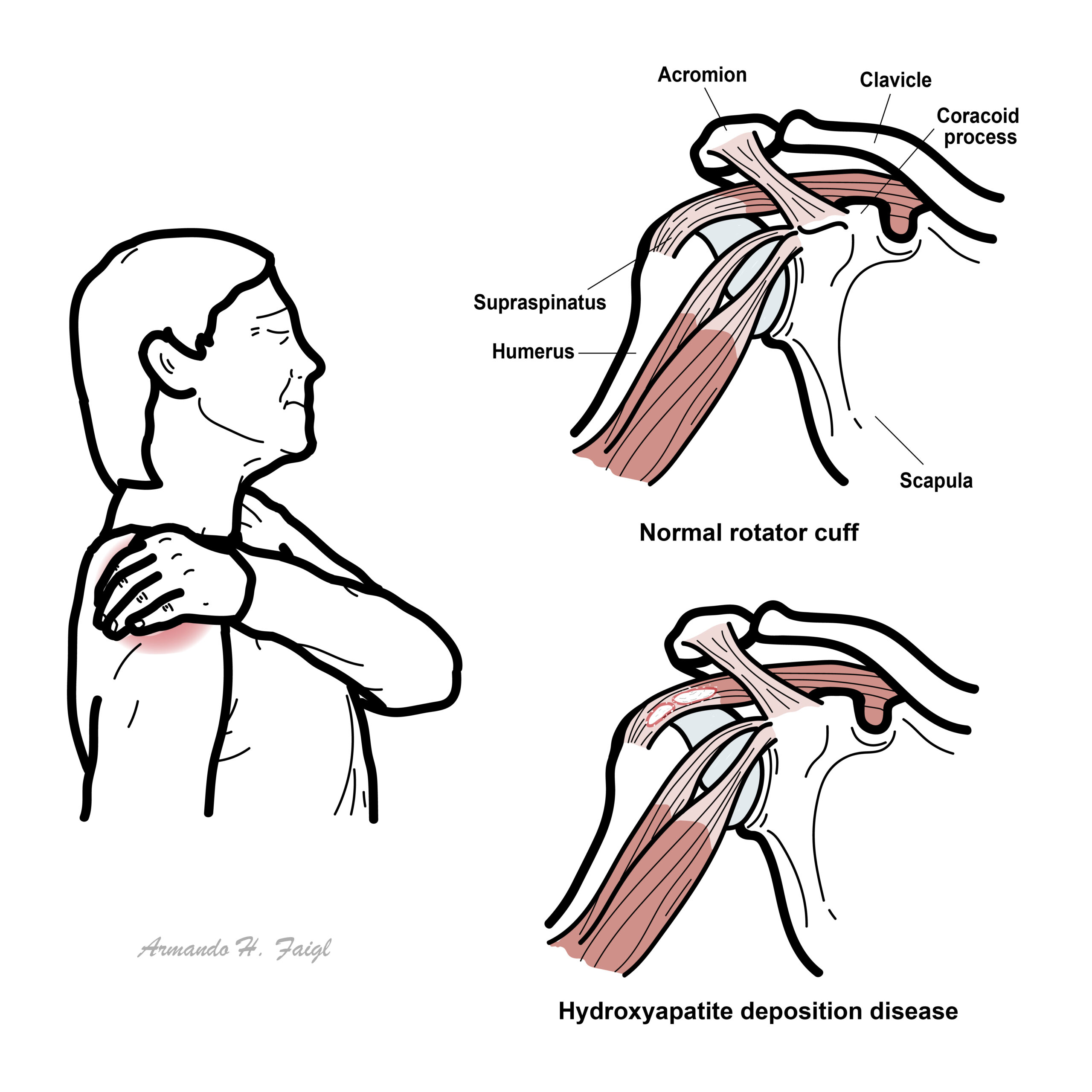
- The rotator cuff (supraspinatus, infraspinatus, subscapularis, teres minor) stabilizes the glenohumeral joint.
- The subacromial-subdeltoid bursa reduces friction between the rotator cuff and overlying structures.
- Tendons are poorly vascularized, especially near insertion zones (enthesis), which may predispose to crystal deposition.
Aetiology and Risk Factors
Aetiology
- Unknown in most cases (idiopathic)
- Possibly due to cell necrosis, hypoxia, or local mechanical stress causing crystal precipitation
- May be related to disordered healing of tendon microtears
- Age 30–60
- Female sex
- Diabetes mellitus
- Hypothyroidism
- Repetitive overuse or trauma (especially shoulder)
- Chronic renal disease (rare)
HADD = middle-aged women + shoulder pain + calcification.
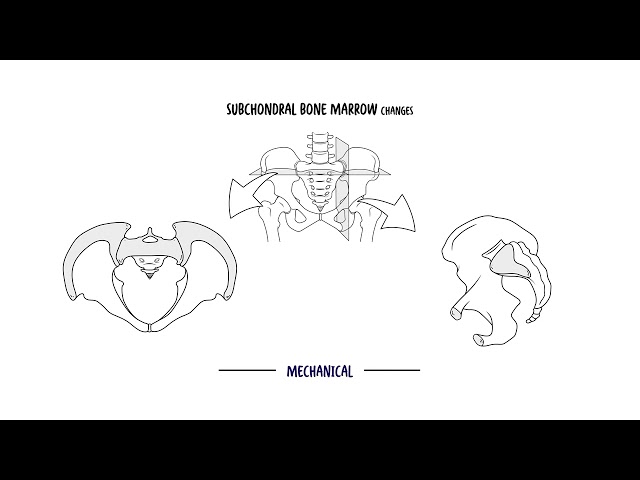
Pathophysiology
- Pre-calcific stage: Fibrocartilaginous metaplasia occurs in tendon → prone to mineralization
- Calcific stage:
- Formative phase: Deposition of HA crystals
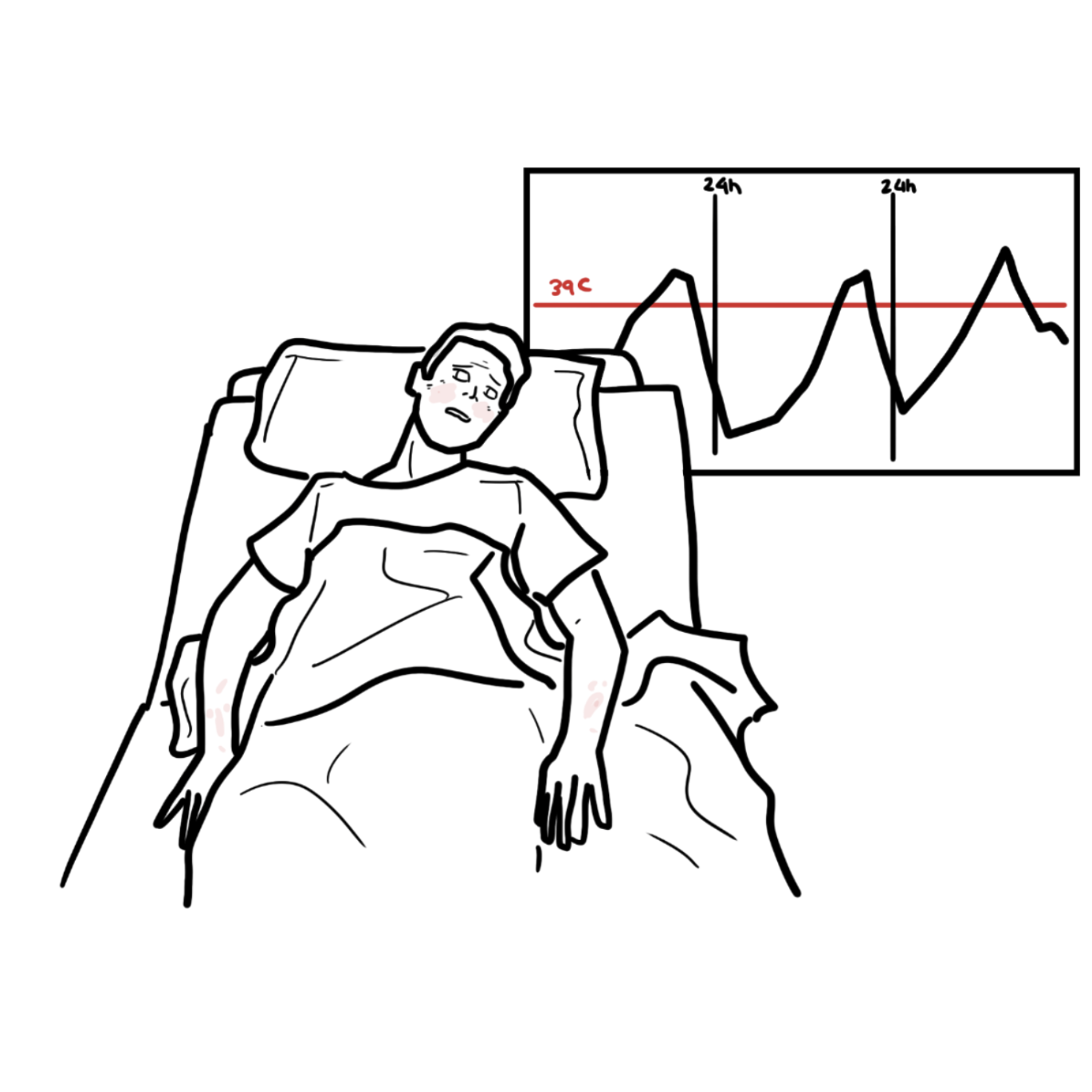
- Resorptive phase: Inflammatory reaction with macrophage and giant cell infiltration → severe pain
- Post-calcific stage: Remodeling and healing with tendon reconstitution
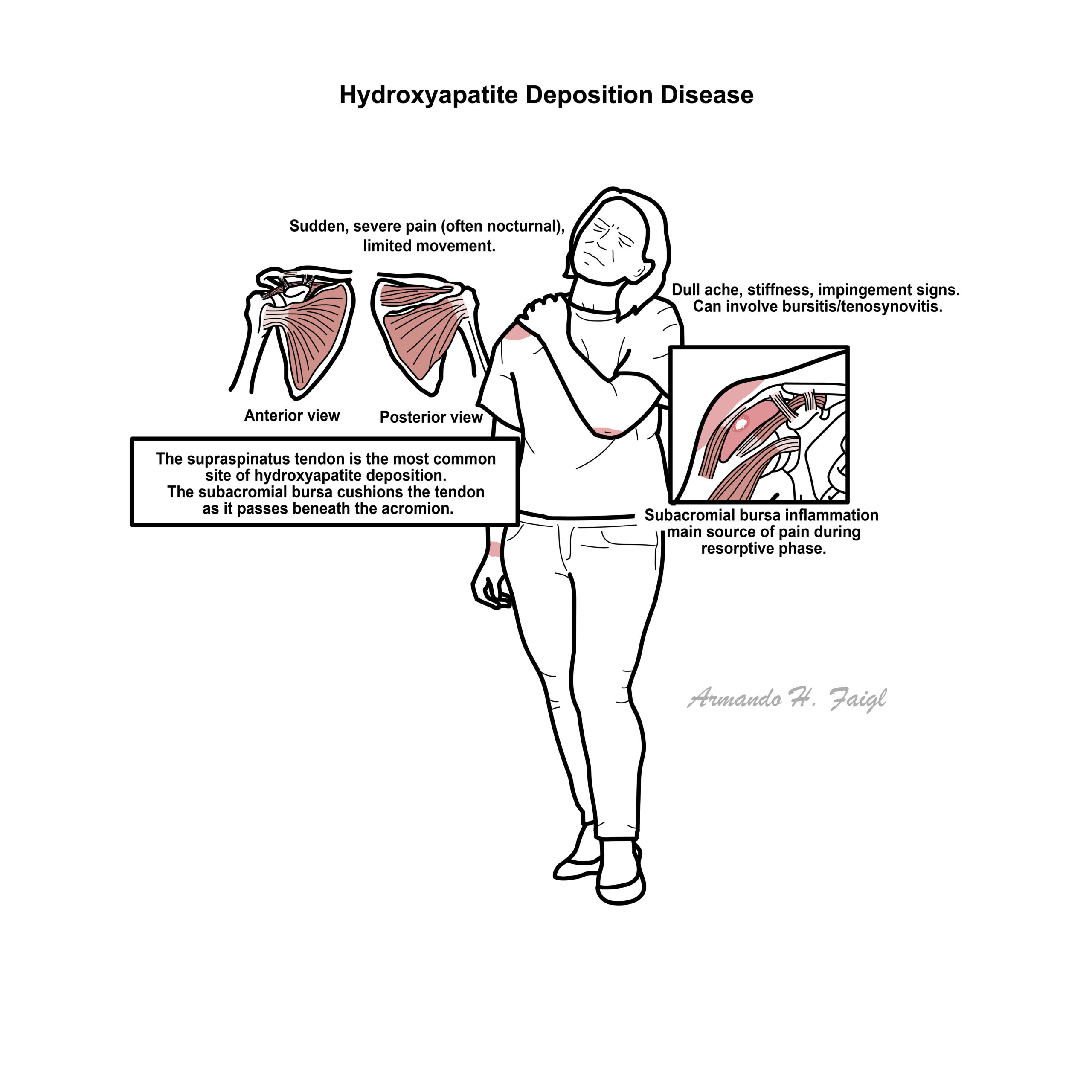
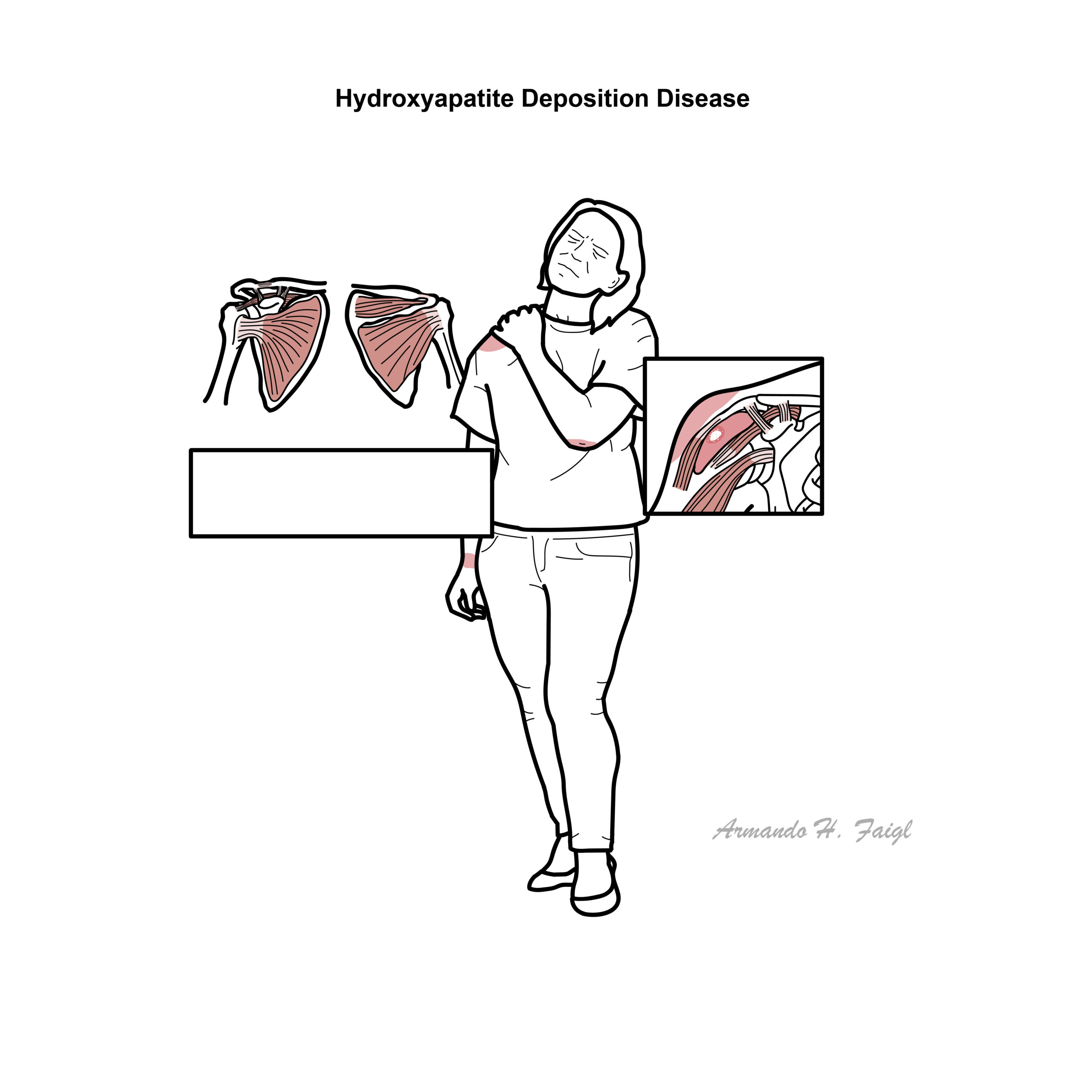
Symptoms typically arise in the resorptive phase due to intense local inflammation.
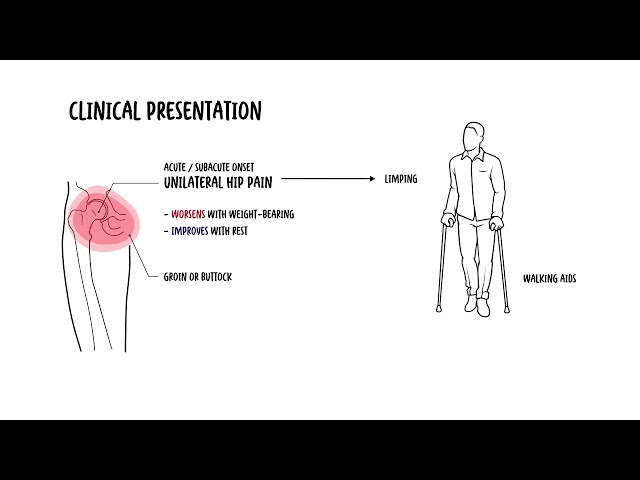
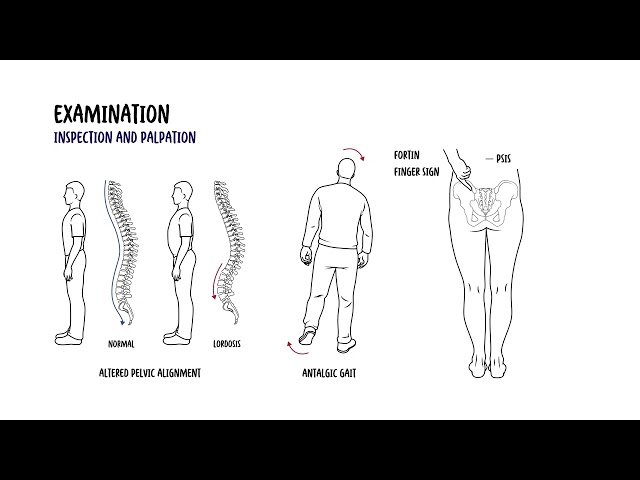
Clinical Manifestations
- Often asymptomatic during formative phase
- Acute calcific tendinitis
- Sudden, severe shoulder pain, often nocturnal
- Limited active ROM, especially abduction and external rotation
- Pain on palpation over greater tuberosity
- Chronic phase
- Dull ache
- Stiffness and impingement signs
- Bursitis or tenosynovitis if crystals rupture into adjacent structures
- Less common sites: hip, elbow, wrist, knee
Shoulder pain + calcification on X-ray + intact ROM = HADD.
Diagnosis
No formal criteria, diagnosis is clinical + radiologic
- X-ray
- Homogeneous, dense calcific deposit in tendon (e.g. supraspinatus)
- Location: 1–2 cm from insertion
- Ultrasound
- Hyperechoic calcification with posterior shadowing
- May show signs of bursitis or tendon rupture
- MRI
- Shows soft tissue edema, inflammation, may mimic rotator cuff tear
- Aspiration (rarely done)
- HA crystals are non-birefringent, not visualized on polarised microscopy
- Can stain with Alizarin red (calcium-binding dye)
Crystal Arthropathy Clinical Comparison Table
| Feature | Gout | Pseudogout (CPPD) | BCP / Milwaukee Shoulder | HADD (Hydroxyapatite) |
| Typical Age | 30–50 (M > F) | >60 | >70 (F > M) | 30–60 (F > M) |
| Crystal Type & Shape | Monosodium urate, needle | Calcium pyrophosphate, rhomboid | BCP (hydroxyapatite), amorphous | Hydroxyapatite, amorphous |
| Birefringence | Strongly negative | Weakly positive | None | None |
| Common Joint Involved | 1st MTP, midfoot, ankle | Knee, wrist | Shoulder (glenohumeral joint) | Shoulder (supraspinatus tendon) |
| Synovial Fluid WBC | High (2,000–50,000+) | Moderate (2,000–50,000) | Low (<2,000), non-inflammatory | Normal to mildly elevated |
Differential diagnoses
- Rotator cuff tear
- Subacromial bursitis
- Adhesive capsulitis
- Septic arthritis (if systemic signs present)
- Gout/pseudogout (if intra-articular)
HADD calcific deposits are dense, homogeneous on X-ray and non-birefringent.
If unsure on ultrasound, confirm with X-ray – classic finding is curvilinear or oval dense calcification near tendon insertion.
Treatment
- NSAIDs (first-line)
- Rest and ice
- Physiotherapy (after acute pain subsides)
- Local corticosteroid injection if significant inflammation
- Needle lavage/barbotage (ultrasound-guided): break up and aspirate calcification
- Ultrasound therapy for pain control
- Surgery (arthroscopic removal) if refractory after 6–12 months
Chronic phase
- Ongoing physiotherapy and ROM exercises
- Treat contributing factors (e.g. diabetes, thyroid dysfunction)
Complications and Prognosis
- Rotator cuff tear
- Adhesive capsulitis
- Chronic pain or impingement syndrome
- Bursal rupture or inflammation
- Excellent prognosis in most with conservative management
- Most resolve spontaneously within 1–3 weeks during resorptive phase
Poor Prognostic Factors
- Large deposits
- Chronic symptoms >6 months
- Recurrent episodes
- Poor compliance with rehab
References
- Harvie P, Pollard TC, Carr AJ. Calcific tendinitis: natural history and association with endocrine disorders. J Shoulder Elbow Surg. 2007;16(2):169–173.
- Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: pathogenesis, diagnosis, and management. J Am Acad Orthop Surg. 1997;5(4):183–191.
- Chianca V, et al. Calcific tendinopathy: imaging findings and therapeutic options. Radiol Med. 2020;125(5):431–447.
- Jiménez-Martín A, et al. Calcific tendinopathy of the shoulder: clinical and radiological analysis of 100 patients. Clin Rheumatol. 2022;41(3):821–828.
- de Witte PB, et al. Therapeutic options for calcific tendinitis of the rotator cuff: a state-of-the-art review. Br J Sports Med. 2016;50(15):884–890.







Members only discussions coming soon…