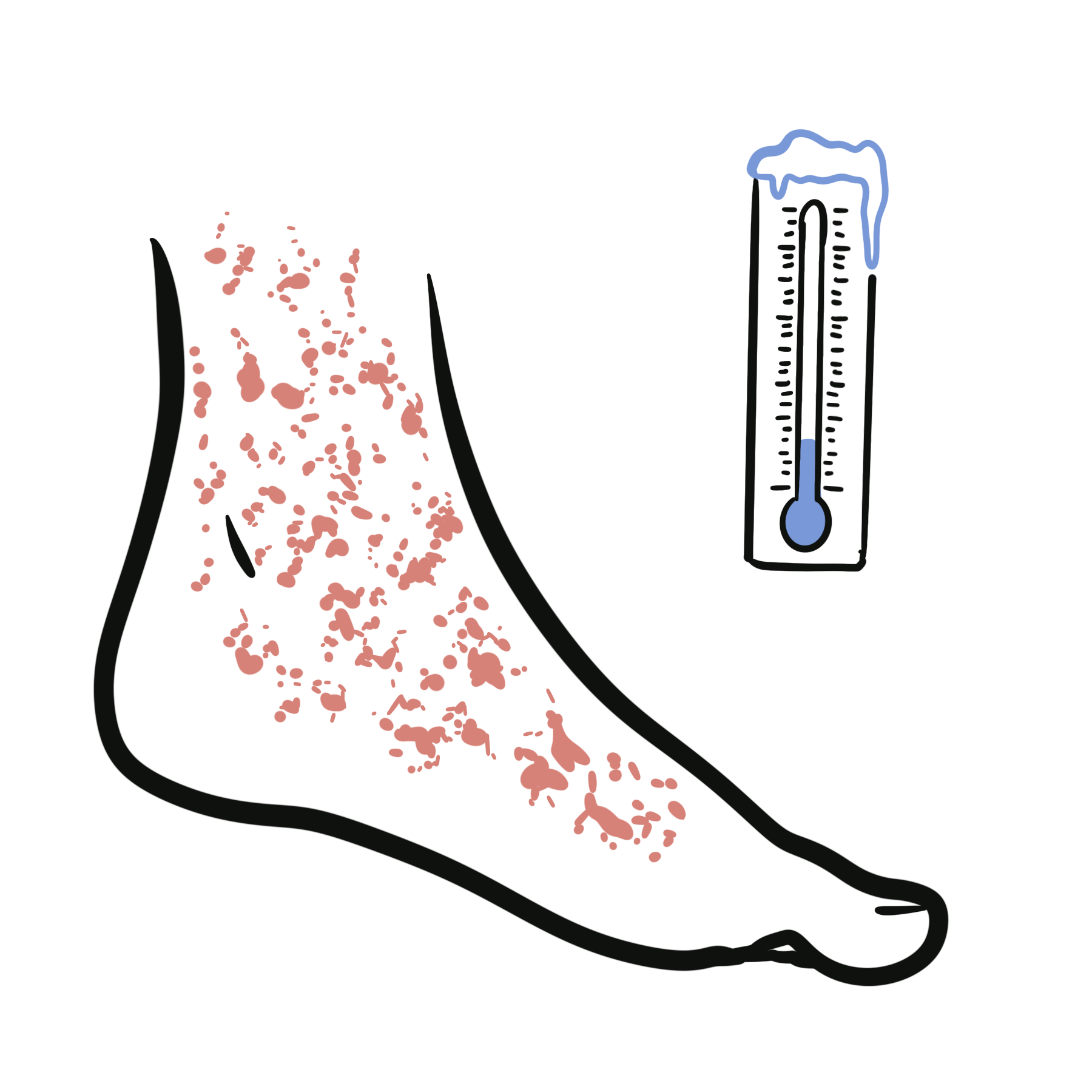
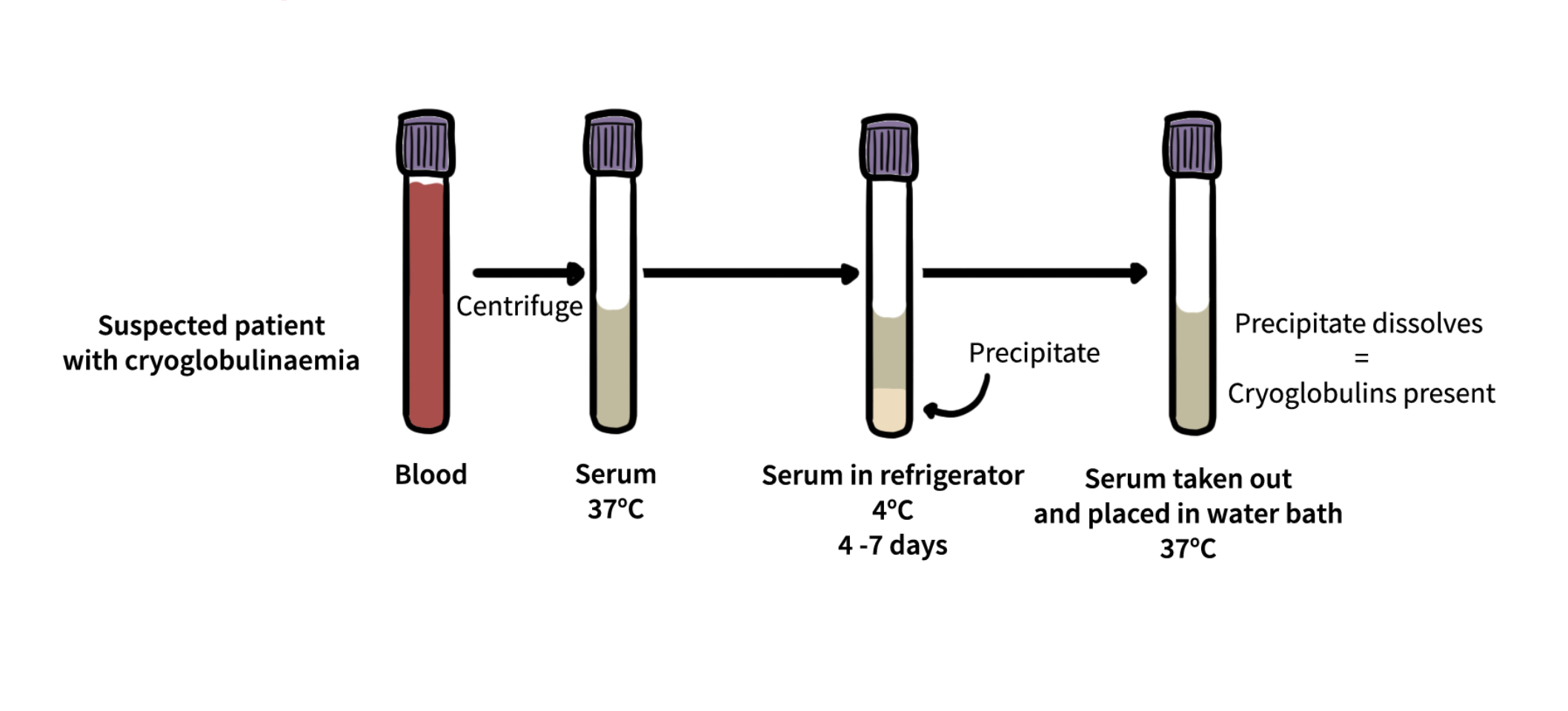
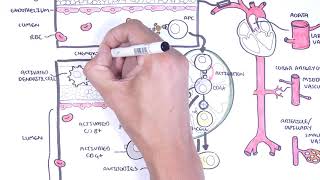
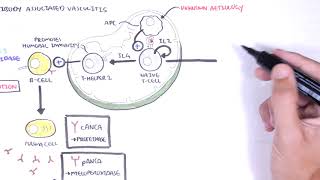
Cryoglobulinaemic vasculitis is an immune complex–mediated small to medium vessel vasculitis caused by circulating cryoglobulins—immunoglobulins that precipitate below 37 °C and redissolve on warming. These immune complexes deposit in vessel walls, activate complement (typically with marked C4 consumption), and drive leukocytoclastic vasculitis. “Mixed” CV (types II and III) is most often linked to hepatitis C virus (HCV), autoimmune diseases, or B-cell clonal disorders, while type I CV is monoclonal and associated with plasma-cell dyscrasias or lymphoproliferative disorders. Adults are most commonly affected.
Definition
Cryoglobulins: Immunoglobulins that precipitate at <37 °C and dissolve on rewarming; quantified as cryocrit (%) and typed by immunofixation into Brouet types I–III. Mixed cryoglobulinaemia: Type II (monoclonal IgM-RF + polyclonal IgG) or Type III (polyclonal IgM-RF + polyclonal IgG); RF activity drives immune complex formation. Type I cryoglobulinaemia: Monoclonal immunoglobulin (IgM or IgG) from a haematologic clone; causes ischemia/hyperviscosity more than vasculitis. Membranoproliferative glomerulonephritis (MPGN): Immune-complex GN typical of mixed CV renal disease.
Always keep blood samples at 37 °C until serum separation to avoid false-negative cryoglobulin results.






















Discussion