
Overview
Acute kidney injury (AKI) (formerly acute renal failure) is the syndrome arising from a rapid fall in GFR (over hours to days). It is characterized by retention of both nitrogenous (including Urea and Creatinine) and non-nitrogenous waste products of metabolism, as well as disordered electrolyte, acid– base, and fluid homeostasis.
Remember
AKI is neither a diagnosis nor a disease. Rather, it is a clinical syndrome that is caused by, or complicates, a wide range of disorders
Definition
Acute Kidney Injury: Rapid reduction in kidney function over hours to days, as measured by serum urea and creatinine and leading to a failure to maintain fluid, electrolyte and acid-base homeostasis.
Chronic Kidney Disease: Impaired renal function >3months based on abnormal structure or function, or GFR <60 for >3months.
Oliguria: A urine output of <400ml/day may be the earlier sign of impaired renal function
Epidemiology
Develop in 5- 20% of hospitalised patients and a significant contributor to morbidity and mortality in the critically ill
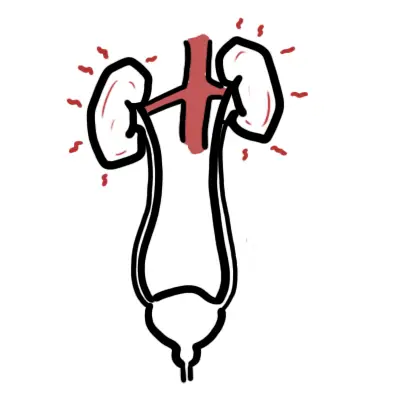
Anatomy and Physiology
Renal Anatomy
The urinary system consists of:
- Kidneys
- Ureters
- Bladder
- Urethra
The kidneys are retroperitoneal bean shaped organs thats sits between veretbral levels T11-L3, the left kidney sitting slightly higher then the right kidney.
The kidneys is divided into three sections:
- Renal cortex – renal arches and renal columns
- Renal Medulla – pyramids, papillae, major calyx, minor calyx
- Renal Sinus – Pelvis, renal vessels and lymphatics
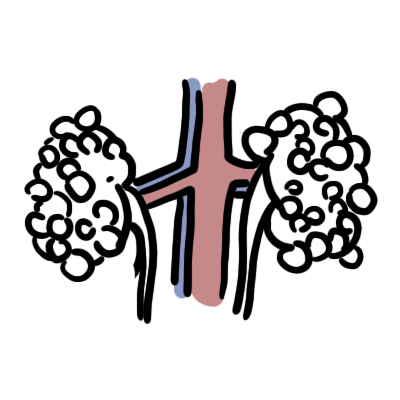
Arterial Supply
- Aorta → Renal artery (L2) → Segmental artery → Interlobular artery → Cortical radiate artery → Afferent Arteriole → GLOMERULUS
Venous Drainage
- GLOMERULUS → Efferent arteriole (has branches forming the Vasa recta) → Arcuate vein → Interlobar vein → Renal Vein → Inferior vena cava
Nephrons
- Functional units of Kidneys
- Nephron’s are structurally divided into two types:
- Cortical
- Juxtamedullary
Ureters are narrow muscular tube that transport urine to the bladder. There are three narrowed areas of each ureter:
- Ureteropelvic junction
- Ureteral segment
- Ureterovesical junction
Bladder is a muscular organ which holds urine. The wall of the bladder comprises of four layers:
- Adventitia
- Detrusor muscle
- lamina propria
- Urothelium – specialised transitional cell epithelium (can stretch)
Urethra Arisis from the base of the bladder and is the passageway through which urine is discharged from the body. The female urethra is much shorter (3-4cm) than the male urethra (18+cm)

Watch Video Nephrology Overview
Renal Physiology
- Regulation of plasma ionic composition
- Regulation of plasma volume
- Regulation of plasma osmolarity
- Regulation of plasma hydrogen ion concentration (pH)
- Removal of metabolic waste products and foreign substance from the plasma.
Classification
AKI Triad Reduced GFR, reduced urine output and increase in nitrogenous waste in blood.

Aetiology and Prevention
The aetiology of acute kidney injury can be simply divided into pre-renal, renal and post renal causes.
Pre-renal – Sepsis and hypotension:
- Severe sepsis
- Haemorrhage
- Dehydration
- Cardiac failure
- Liver failure
- Renovascular insult
Intrarenal
- Toxicity:
- Nephrotoxic drugs
- Iodinated radiological contrast
- Parenchymal kidney disease:
- Glomerulonephritis
- Tubulointerstitial nephritis
- Rhabdomyolysis
- Haemolytic uraemic syndrome
- Myeloma
- Malignant hypertension
Post renal Obstruction:
- Bladder outflow
- Stones
- Tumour
- Surgical ligation of ureters
- Extrinsic compression (lymph nodes)
- Retroperitoneal fibrosis
Investigations
- Urine Dipstick
- FBC
- Clotting profile
- Group and save – if anaemia
- CRP/ESR
- Blood smears
- EUC
- LFTs
- CK – rhabdomyolysis?
- Urate – tumour lysis syndrome?
- Lactate – tissue ischaemia?
- Blood culture
- Arterial blood gas
- CMP
Remember
Percuss the bladder and perform bladder ultrasound in case the reason for oliguria is bladder in origin.
Screening for nephritis/nephrotic syndromes
- Anti-ANA
- ANCA
- Anti-GBM
- Anti-streptolysin O tites
- Protein electrophoresis
- Immunoglobuins (IgG, IgA and IgM
- Rheumatoid factor
- Viral serology – HIV, HBV, HCV
- Antiphospholipid syndrome
Imaging
- Renal ultrasound
- Chest X-ray – pulmonary oedema? pulmonary infection?
- Renal scans
- MAG 3 scan
- Renal biopsy
Management
Overview Initial treatment should focus on correcting fluid and electrolyte balances and uremia while the cause of acute renal failure is being sought. A volume-depleted patient is resuscitated with saline. The main electrolyte disturbances in the acute setting are hyperkalemia and acidosis.
General
- Fluid Replacement – The key to achieving euvolaemia is repeated clinical assessment of a patient’s volume status
- Review medications and stop nephrotoxins
- Monitor and adjust diet
Treat underlying cause
- Prerenal
- Intrarenal
- Postrenal
Treat complications
- Hyperkalaemia
- Calcium gluconate – it does not ↓potassium but is cardioprotective
- Insulin and glucose
- Sodium bicarbonate
- B2 agnoists – Salbutamol
- Urinary K+ wasting: diuretics
- Gut K+ wasting: exchange resins
Remember
Hyperkalaemia can induce cardiac dysrhythmias with the following ECG changes: Peak T waves (tenting), flattening of P waves and prolonged PR interval
- Pulmonary Oedema
- Sit patient up
- Oxygen
- Opiates
- Nitrates
- Diuretics
- Hyperphosphataemia
- Dietary restriction of phosphate
- PO4 removal through dialysis or haemofiltration.
- Oral phosphate binder (calcium carbonate)
- Hypocalcaemia
- Calcium is supplemented orally
Remember
In rhabdomyolysis, Ca2+ can precipitate in injured muscle, causing necrosis and ischaemic contractures—resist the administration of Ca2+ unless symptomatic hypocalcaemia.
- Hypomagnesaemia
- Magnesium supplement
- Anaemia – Bleeding?
- Infections – Antibiotics
Side note
Side note Sepsis is an important cause of morbidity and mortality in AKI (75% mortality if AKI + sepsis).
| Indications for Dialysis (AEIOU) |
| Acidosis |
| Electrolytes – refractory hyperkalaemia |
| Ingestions/intoxication – Barbiturates, lithium, alcohol, salicylates, theophyline |
| Overload – Pulmonary oedema |
| Uraemia Complications – pericarditis, refractory pulmonary oedema and encephalopathy |
Summary

Complications
- Electrolyte imbalance
- Hyperkalaemia
- Pulmonary oedema
- Uraemic complications
- Reduced conscious level
Remember
Hyperkalaemia can induce cardiac dysrhythmias with the following ECG changes: Peak T waves (tenting) → flattening of P waves and prolonged PR interval


Discussion