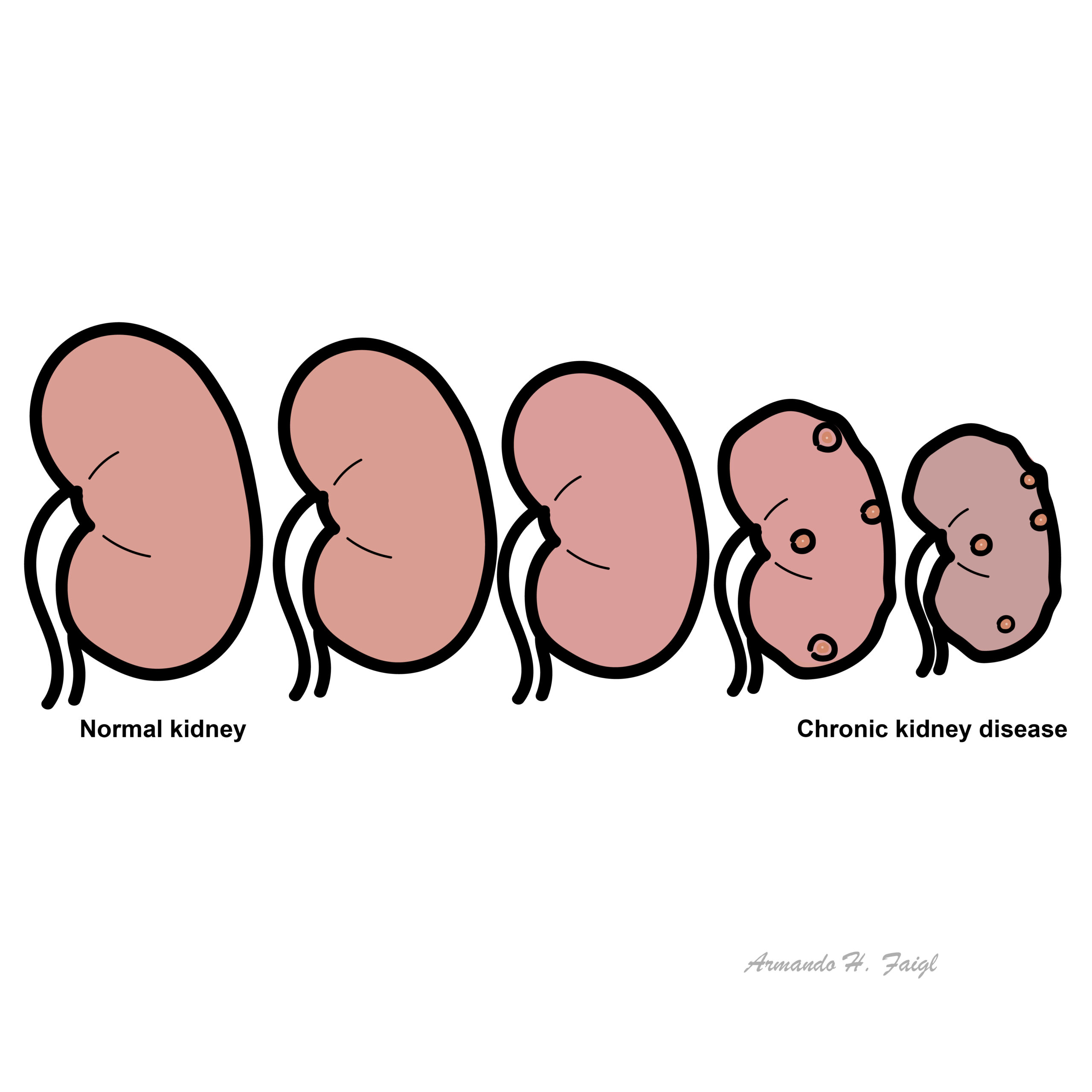
Chronic Kidney Disease

CKD is responsible for a substantial burden of illness and premature death. The kidneys are basically not working as good.
Always assume a ↓ eGFR represents acute kidney injury until proven otherwise.
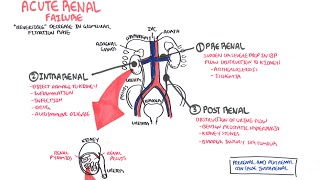
Acute Kidney Injury: Rapid reduction in kidney function over hours to days, as measured by serum urea and creatinine and leading to a failure to maintain fluid, electrolyte and acid-base homeostasis.
Acute Kidney Failure:
Chronic Kidney Disease: Impaired renal function >3months based on abnormal structure or function, or GFR <60 for >3months with evidence of kidney dysfunction.
| Limitations to eGFR |
| Accurate to +/- 30% |
| Not for use in children, pregnancy, dialysis |
| Extremes of body composition and size |
| Vegetarian diets |
| Rapidly changing renal function |
| Interferences with creatinine assays |
If eGFR is < 60 mL/min/1.73 m2, consider clinical situations where eGFR results may be unreliable and/or misleading and retest within 14 days. GFR (mL/min) = GFR (mL/min/1.73m²) x BSA / 1.73.
Diabetic Nephropathy
Overview
Type II diabetes Mellitus is the leading cause of Chronic Kidney Disease. It is classified as a secondary nephrotic syndrome. 20% of people with Type II diabetes will develop end stage kidney disease. Everyone with Diabetes should be screened yearly for microalbuminuria.
Clinical features – Nephrotic Syndrome with signs and symptoms of diabetes (hyperglycemia)
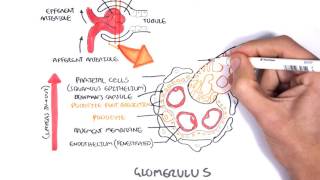
Pathological features Diabetic kidney disease is defined by characteristic structural and functional changes. The predominant structural changes include
| Staging | |
| Class I | Isolated glomerular basement membrane thickening. There is no evidence of mesangial expansion, increased mesangial matrix, or global glomerulosclerosis involving >50 percent of glomeruli. |
| Class II | Mild (class IIa) or severe (class IIb) mesangial expansion. |
| Class III | At least one Kimmelstiel-Wilson lesion (nodular intercapillary glomerulosclerosis) is observed on biopsy and there is <50 percent global glomerulosclerosis. |
| Class IV | Advanced diabetic sclerosis. There is >50 percent global glomerulosclerosis. |
Management and Prognosis Microalbuminuria is reversible if caught early and managed vigorously.
More info on Long-Term Complications of Diabetes Type II
Proteinuria, which is a clinical marker for CKD, is also indicative of an increased risk of cardiovascular disease.
Patients with CKD are often asymptomatic until the advanced stages
Severe Chronic Kidney Disease (GFR <20mL/min)
Examination
Common causes of Chronic Kidney Disease
Determining Renal Function
Determine renal structure
Assess effects of Chronic Kidney Disease on body
| Stage | eGFR ml/min/1.73m² |
| Stage 1 | >90 (Normal) |
| Stage 2 | 60-90 (Mild) |
| Stage 3a | 45-60 (Moderate) |
| Stage 3b | 30-44 (Moderate) |
| Stage 4 | 15-29 (Severe) |
| Stage 5 | <16 (End-Stage) |
The majority of patients with CKD stages 1–3 do not progress to kidney failure. The risk of death from CV disease is far higher than the risk of progression. Mild to moderate CKD is usually managed in general practice or by other physicians caring for the patient. Referral to nephrologist should be considered if:
Normal GFR is >90mL/min/1.73m² (130L/day).
Low eGFR and raised urine albumin are markers for death, CVD, End-Stage Kidney disease, Acute Kidney Injury.
General and limit progression/complication of CKD
CKD with hyperkalaemia be careful with using ACE inhibitors or K+ sparing diuretics.
Symptomatic treatment (usually associated with uraemia)
Treat complications
Preparation for renal replacement therapy
Dialysis
| Indications for Dialysis (AEIOU) |
| Acidosis |
| Electrolytes – refractory hyperkalaemia |
| Ingestions/intoxication – Barbiturates, lithium, alcohol, salicylates, theophyline |
| Overload – Pulmonary oedema |
| Uraemia Complications – pericarditis, refractory pulmonary oedema and encephalopathy |
Complications
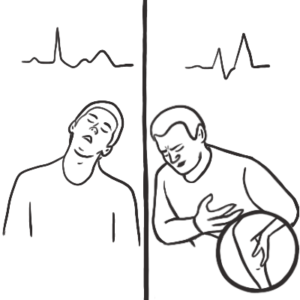
Hyperkalaemia on ECG is characterised by Peak T wave and later widened QRS complex.
Hypocalcaemia on ECG is charactersied by QT complex prolongation primarily by prolonging the ST segment. No change is T wave.
UpToDate
Best Practice
Davidson’s Principles and Practices of Medicine













Discussion