

Bladder Carcinoma

Mainly focusing on Transitional cell tumours
Overview
| Three main types of bladder carcinoma |
| Transitional cell carcinoma (Most common) |
| Squamous cell carcinoma |
| Adenocarcinoma (Rare) |
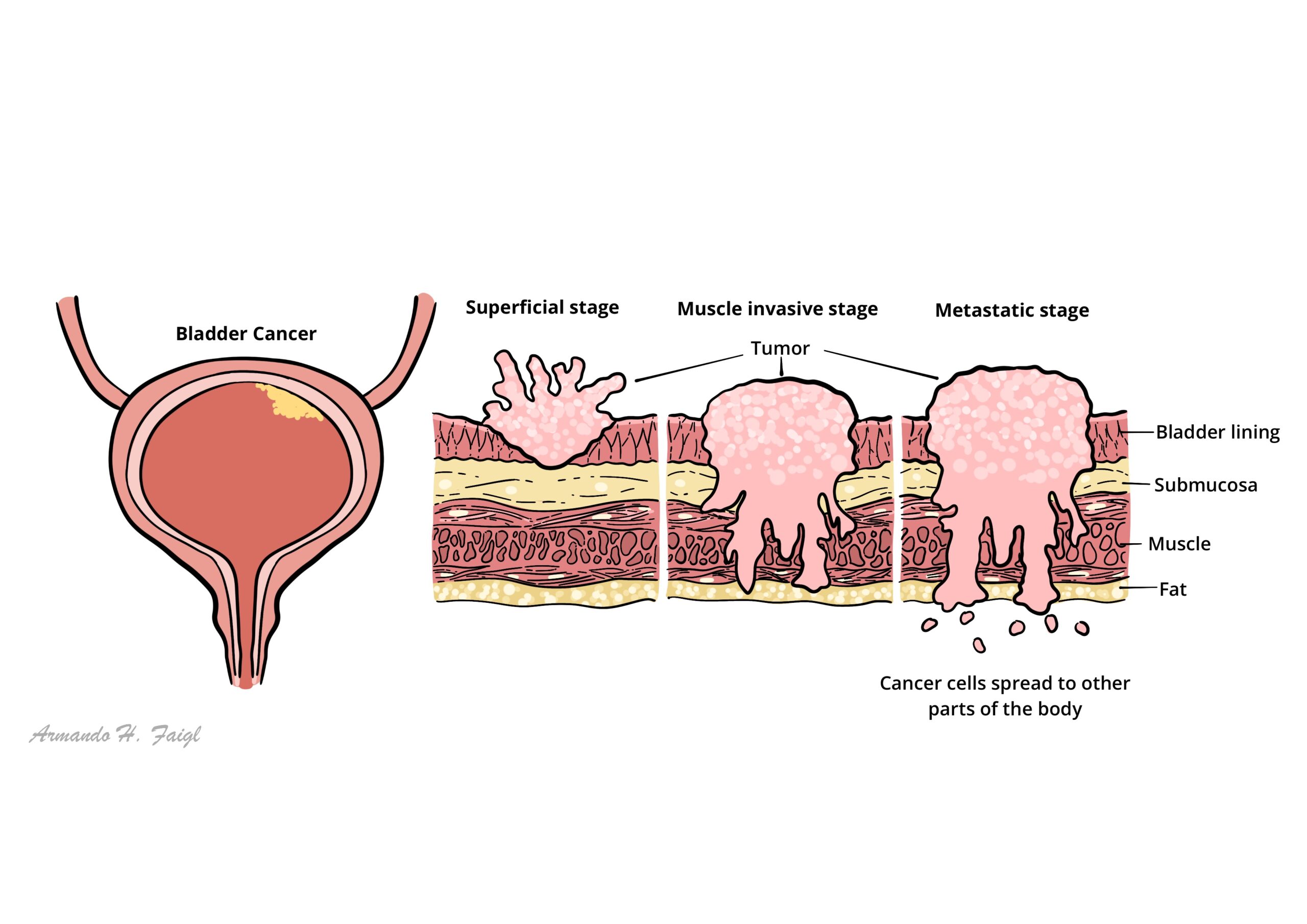
Transitional cell tumours can affect any part of the urinary epithelium. It is the second most common urological malignancy (Renal Adenocarcinoma is the most common, bladder adenocarcinoma is rare) and is one of the most common cause of cancer related death. Bladder cancer occurs most commonly from the fifth to seventh decades of life and is more common in men. Transitional cell tumour is also known as urothelial carcinoma and has a broad spectrum of morphology from low grade, sea weed looking, superficial papiliferous growths to invasive, solid mass.
Definition
Transitional endothelial cells: Endothelial cells that can change shape
Transitional cell Tumours (TCT): Spectrum of disease from benign superficial growths to invasive carcinomas. TCTs may affect any part of the urinary epithelium (bladder, ureter).
Transitional epithelial cells are found in the bladder, ureter and part of the kidneys and urethra. Therefore transitional cell carcinoma can occur in any of these areas.
Bladder Anatomy & Physiology
An empty urinary bladder sits behind the pubic symphysis, when filled the bladder rises and is higher and can be readily palpated and percussed. In children the urinary bladder sits higher normally.
Extending of the dome of the bladder to the umbilicus is the median umbilical ligament, a fibrous cord that represents the obliterated urachus.
Layers of the bladder
- Urotherlium (transitional cells)
- Basement membrane
- Lamine propria (Connective tissue)
- Detrusor muscle (inner and outer layer)
- Adventitia (fat)
- Visceral peritoneum
Detrusor muscle is made up of smoother muscle fibers arranged at random in a longitudinal, circular and spiral manner without any layer formation or orientation. However at the internal meatus, the detrusor muscle forms three specific layers:
- Inner longitudinal
- Middle circular
- Outer longitudinal
Arterial Supply
- Superior vesical artery
- Middle vesical artery
- Inferior vesical artery
- Obturator artery
- Inferior gluteal artery
In females the uterine and vaginal artery also send some blood supply
Venous drainage Surrounding the bladder is a rich venous supply that drains essentially to the internal iliac veins → common iliac veins → IVC
- Vesical lymph nodes
- Common iliac lymph nodes
- Internal iliac lymph nodes (hypogastric)
- External iliac lymph nodes
Innervation
- Parasympathetic nerves (S2, S3, S4) → promotes urination
- Sympathetic nerves (T11, T12, L1, L2) → inhibits urination
- Somatic nerves (voluntary control) → controls external sphincter (holding in urine)
Micturition Physiology
Risk Factors
| Risk Factors |
| Age >40 years old |
| Smoking (main factor) |
| Aromatic amines |
| Cyclophosphamide |
| Schistosoma haemotabium (squamous cell carcinoma) |
| Chronic irritation (squamous cell carcinoma) |
| Aristolochic acid |
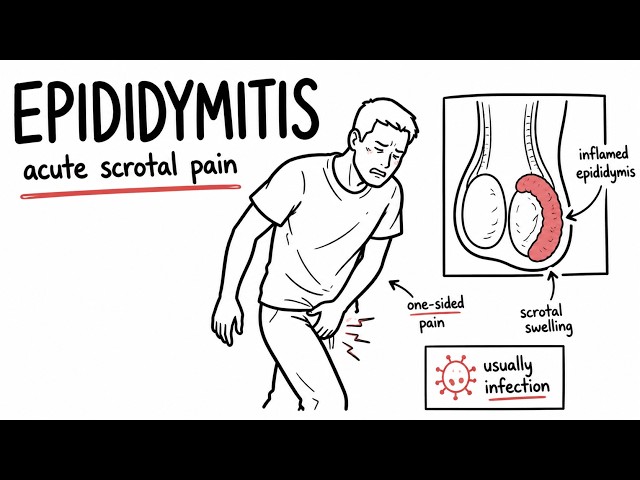
Clinical Manifestation
The most common presentation of bladder cancer is painless haematuria.
Painless haematuria: Microscopic (invisible) or macroscopic
Irritative symptoms
- Dysuria (Painful micturition)
- Frequency
- Urgency
- Renal colic due to blood clot
Obstructive symptoms
- Feeling of incomplete voiding
- Double voiding
Signs and Advanced disease
- Constitutional signs and symptoms
- Suprapubic palpable mass
>40 year old presenting with painless haematuria is bladder malignancy (+/- risk factors) until proven otherwise.
All patients with macroscopic haematuria or persistent microscopic haematuria should be referred to a urologist for evaluation.
- Renal Cell Carcinoma
- Prostate Cancer
- Benign Prostate Hyperplasia
- Urinary stones/Nephrolithiasis
- Urinary Tract Infection
- Urethral strictures
Investigation
- Urine cytology (urine cell analysis) – Checks for malignant cell. If present likely to be malignancy. If not present can still be low-grade tumour and needs cystoscopy to confirm
- Cystoscopy – carried out by flexible cystoscope and can visualise the bladder lining. It is gold standard.
Classification & Staging
| WHO Grading of transitional carcinoma |
| Urothelial papilloma |
| Papillary urothelial neoplasms of low malignant potential (PUNLMP) |
| Low-grade papillary urothelial carcinoma (PRESENTS MOST COMMON) |
| High-grade papillary urothelial carcinoma |
Staging uses MRI and CR scanning to detect local or systemic spread.
To make it easy think of Low-grade as being non-muscle invasive and high grade as muscle invasive.
Pathology
70% are superficial in nature at diagnosis, being confined to the mucosa. Transitional cell carcinoma must be differentiated from other forms of bladder cancer
| Bladder Carcnoma | Pathological change |
| Transitional cell carcinoma (most common) | papiliferous growths “seaweed” to solid, invasive looking tumour |
| Squamous cell carcinoma | |
| Adenocarcinoma (rare) |
Transitional carcinoma can invade the muscle layer of the bladder and this will tailor management:
- Nonmuscle invasive bladder cancer
- Muscle invasive bladder cancer
Treatment
| Bladder Carcnoma | Management |
| Transitional cell carcinoma (most common) | Transurethral resection +/- Chemotherapy +/- Radical cystectomy |
| Squamous cell carcinoma | Cystectomy or radiation therapy |
| Adenocarcinoma (rare) | Cystectomy or partial cystectomy + Chemotherapy |
- Nonmuscle invasive bladder cancer can be treated endoscopically
- Muscle invasive bladder cancer best treated with cystectomy
Follow-up
- Postcystectomy patients require 6 monthly contrast enhanced abdominal and pelvic CT scans and chest X-ray (or CT).
- Renal function should also be monitored as strictures can occur in the anastomosis between ureter and ileal conduit or neobladder.
Complications & Prognosis
- Prostatic urethral transitional cell carcinoma
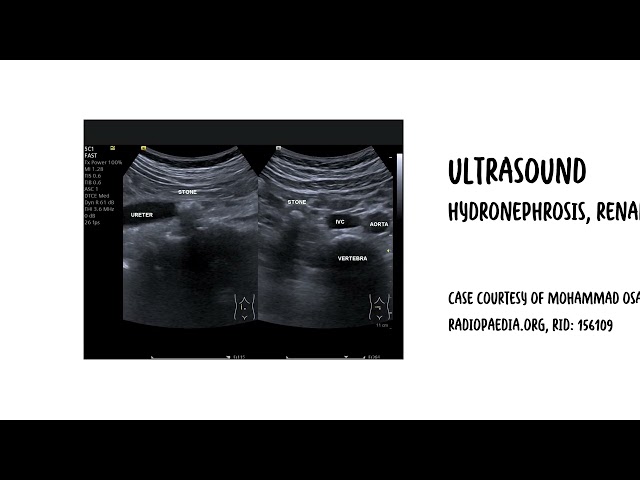
- Hydronephrosis
- Urinary retention
- Complications of Surgery
- 30% develop muscle-invasive disease
- 5 year survival rate for muscle-invasive is 50%
- Metastatic TCT has poor prognosis with a medial survival of 13months
References
Best Practice
Sharma, S, Ksheersagar, P & Sharma, P 2009 Diagnosis and treatment of Bladder Cancer, American Family Physician, vol. 80, no. 7, pp. 717-723.



Members only discussions coming soon…