Overviews
Maternal infections is a broad term for any infection that is acquired by a pregnant woman antepartum, intrapartum or postpartum. These infections may have detrimental impacts on the mother and the foetus/newborn.1 Maternal infections covered in this page include TORCH infections as well as Group B Streptococcal infection and chorioamnionitis.
TORCH infections are a group of congenital infections that can be passed on from the mother to the foetus or newborn. TORCH stands for:
T: toxoplasmosis
O: Other
Syphilis, HIV , Hepatitis B, VZV, Parvovirus B19
R: rubella
C: cytomegalovirus
H: herpes simplex virus
Highest risk to fetus if infection occurs in the first trimester.
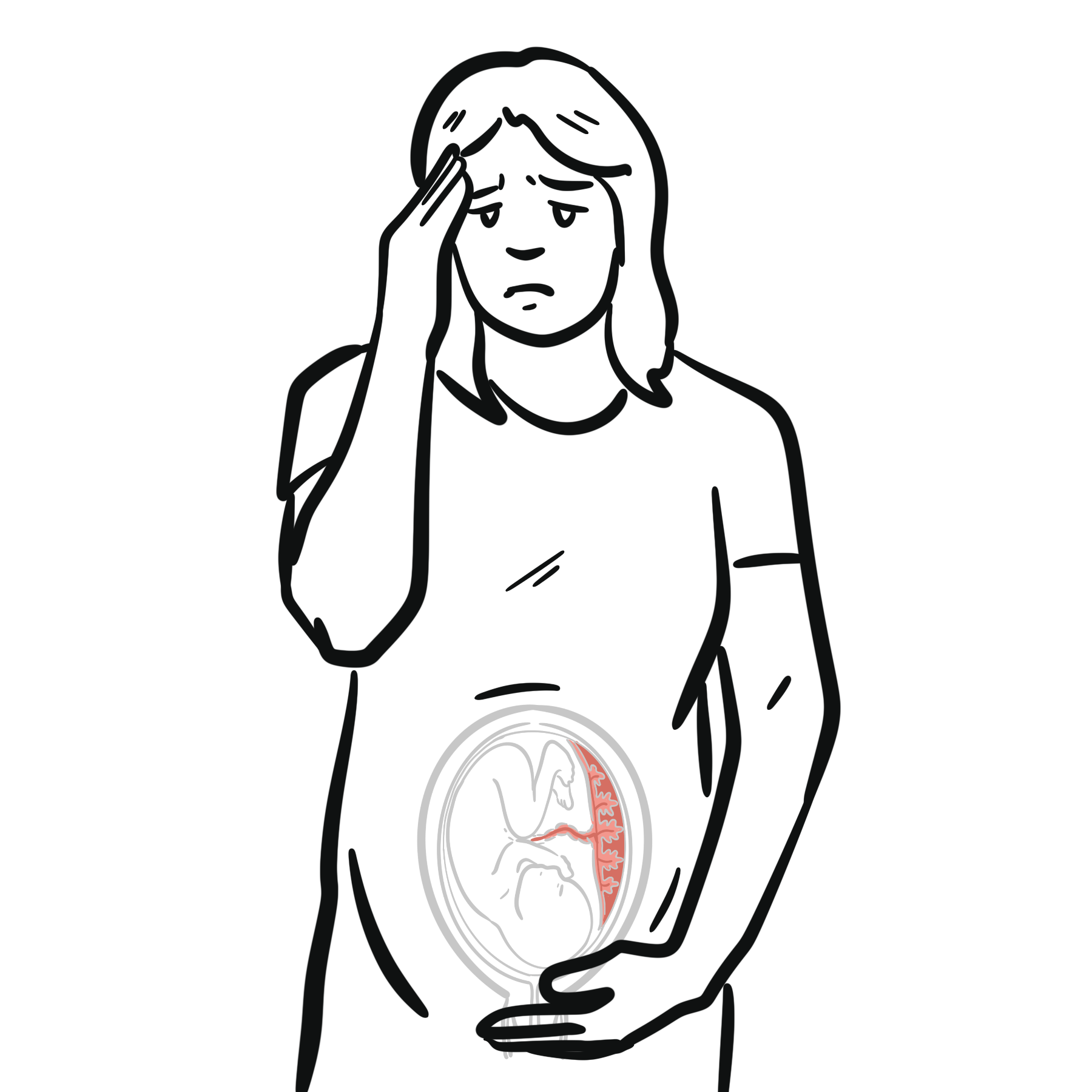
Toxoplasmosis2
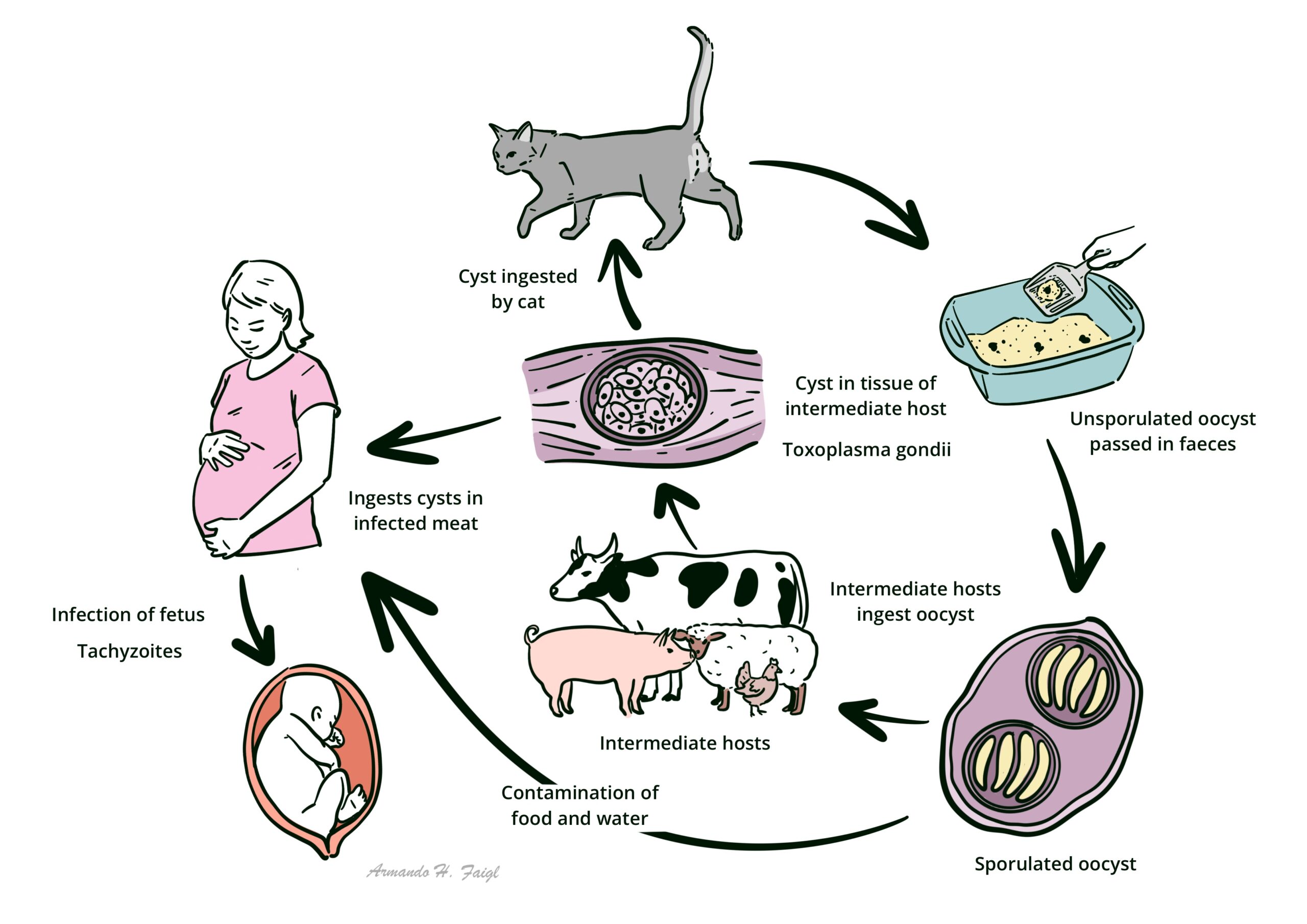
Organism: Toxoplasma gondii – protozoan parasiteCauses
Consumption of raw/inadequately cooked meat infected with cysts
Consumption of food/water contaminated by cat faeces
Transmission/life cycle 3
Incubation period: 5-23 daysMain host: domestic cats
Cats acquire T.gondii through consuming small infected rodents and birds, or cat faeces consumption
The parasite infects the intestinal tract allowing for the sexual stage of the life cycle. Oocytes are then excreted in faeces for 10-20 days
Maternal clinical manifestations
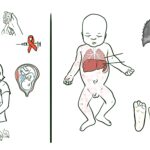
Foetal/neonatal clinical manifestations
Prematurity Neurological triad: hydrocephalus, chorioretinitis, periventricular calcifications
Mental retardation
“blueberry” rash
Jaundice Hepatosplenomegaly
Myocarditis pneumonitis
Investigations
Ix for maternal infection: Serum IgG measurement – serial measurements
Ix for foetal infection: PCR on amniotic fluid
If positive
Ultrasound: to detect any foetal abnormalities
Amniocentesis for PCR at 18-20 weeks gestation, or if >3 weeks after maternal infection identified
Management 4
Spiramycin (brand name – rovamycine)
If <12 weeks gestation: if amniocentesis PCR positive, consider counselling regarding termination of pregnancy
If 28-42 weeks: if spiramycin unavailable → atovaquone or azithromycin
Prevention
Avoid raw/undercooked meat
Wash hands thoroughly after gardening or handling raw meat handling cat litter OR delegate task to others in family,
Wash fresh produce thoroughly before consuming
Syphilis5
Overview: syphilis is a common STI, though if left untreated in a pregnant woman, she can transmit this infection to the unborn infant. Organism
Transmission 6
Unprotected oral, vaginal or anal sex with a person who has become infected
Skin-to-skin contact with syphilis rash
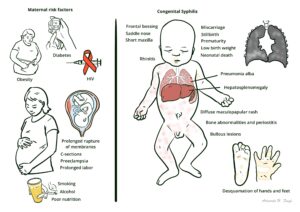
Risk factors
Maternal drug abuse
Homelessness
Low SES
Sex with multiple partners
Failure to receive prenatal care, STI testing
Maternal clinical manifestations
Primary syphilis: painless chancre
Secondary syphilis: fever , generalised lymphadenopathy, maculopapular rash
Late latent syphilis: asymptomatic
tertiary syphilis: gumma, neurosyphilis and cardiovascular syphilis
Foetal/neonatal clinical manifestations
most asymptomatic at birth
early stages: rhinitis, maculopapular rash, lymphadenopathy
later:
facial changes: frontal bossing, saddle nose, short maxilla
anaemia and thrombocytopaenia
Miscarriage
Stillbirth
Prematurity
Low birth weight Neonatal death
Hepatomegaly
Investigations 5
Syphilis serology: all pregnant women
Routine antenatal screening “booking bloods”: <10 weeks gestation
Repeat at 26-28 and 36 weeks gestation
If lesions/chancre present → dry swab syphilis PCS and serology
Management 5
Dependent on the stage of syphilis
Infectious syphilis: benzathine benzylpenicillin 1.8g IM once only
Late latent or unknown duration: benzathine benzylpenicillin IM 1.8g weekly for 3 weeks
Prevention
Using barrier contraception (condoms)
This image series is only available to members
HIV7, 8
Overview
Transmission of HIV from mother to child can occur antepartum, intrapartum, or postpartum (breastfeeding ). Majority of cases occur intrapartum
Organism: Human immunodeficiency virusTransmission : exchange of bodily fluids: blood, semen, vaginal fluids, breast milkMaternal clinical manifestations 9 infant clinical manifestations 8 Investigations 7
Booking bloods: HIV
Baseline bloods: eLFTs, anylase, HLA, FBC ,
CD4 cell count, HIV viral load, HIV resistance testing
Consider low vaginal swab for other STIs
Management 7
Strongly discourage breastfeeding
Consider cabergoline (lactation suppressor)
prescribe anti-retroviral therapy: with consultation with infectious disease
for baby: zidovudine prophylaxis within 6-12 hours of birth, continue for 4 weeks
Hepatitis B
Overview: infection which causes both acute and chronic liver disease . Infants may be infected with this maternal infection primarily during the intrapartum period. Organism: hepatitis B virusTransmission 10 :
broken or penetrated skin, mucosal contact with bodily fluids: blood, saliva, vaginal fluids and breastmilk. Unprotected sex, use of contaminated syringes for illicit drug use, tattooing, body piercing, needle stick injuries
Risk of perinatal transmission is dependent on the level of hep B e antigen in the maternal serum.
Maternal clinical manifestations 11
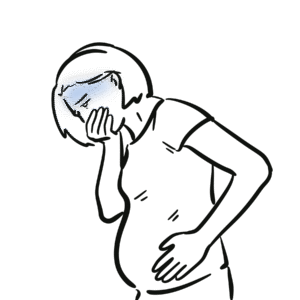
May be asymptomatic
Nausea , anorexia, abdominal pain or discomfort, fatigue, myalgia , dark urine, jaundiceChronic hepatitis infection may lead to: ascites, coagulopathy, thrombocytopaenia, oesophageal varices,
Foetal/neonatal clinical manifestations 12 Investigations
Booking bloods: hepatitis B surface antigen
If positive in booking bloods
LFTs , INR , platelets, complete hepatitis serology, HBV DNA viral load, HIV serology
At 26-28 weeks
Repeat HBV DNA viral load
Management 10
Dependent on HBV DNA viral load
If <200,000 IU/ml → hepatitis B vaccine and hepatitis B immunoglobulin to infant within 12 hours of birth
If > 200,000 IU/ml → tenofovir disproxil fumarate for mother, hepatitis vaccine and hepatitis B immunoglobulin to infant within 12 hours of birth
Prevention 10
Vaccination
Safe sex practices
Varicella Zoster Virus
Overview 13 :
Varicella zoster virus (chickenpox) is part of the herpes family. It is highly contagious.
Organism:
Transmission 13
Respiratory droplets
Direct contact with fluid from vesicles or indirectly via fomites (clothes, hair, skin cells, bedding)
Maternal clinical manifestations 13
Fever
Malaise Pruritic rash: maculopapular → vesicular that crust over
Severe chickenpox
Respiratory symptoms
Haemorrhagic rash or bleeding
New pocks developing after 6 days of infection
Persistent fever >6 days
Neurological symptoms
Congenital varicella syndrome clinical manifestations 14
Skin scarring lesions (cicatrix)
Limb hypoplasia, atrophy
Malformed digits
Ocular defects: chorioretinitis, cataracts, nystagmus
CNS abnormalities: microcephaly, cortical atrophy, seizures, mental retardation
Autonomic nervous system dysfunction: neurogenic bladder, hydronephrosis, reflux, oesophageal dilaiton
Investigations
Serology of antibody status (VZV-IgG)
Management 15
If significant exposure to VZV (>15 minutes in the same space as someone infected with VZV) → varicella zoster immunoglobulin
If mother positive in gestation
If they present within 24 hours of onset of the rash and >19 weeks gestation → give acyclovir PO 800mg 5x 7 days
If > 24 hours: monitor and no aciclovir
Severe chickenpox → IV acyclovir 10mg/kg 8 hourly 7-10 days
For infant
If mother had chickenpox 7 days before – 2 days after birth
Give high titre varicella zoster immunoglobulin (ZIG) 200 IU IM ideally within 24 hours of birth or within 72 hours or birth
If positive in infant
<37 weeks at birth: give IV acyclovir
37 weeks or greater: monitor for respiratory symptoms at home or paediatric unit
Prevention
Vaccination pre-pregnancy
Parvovirus B1916
Overview: also known as slapped cheek syndromeOrganism: Parvovirus B19Transmission
Contact with respiratory secretions
Hand mouth contact
Mother → foetus
Transfusion of blood and blood products
Maternal clinical manifestations
Erythematous rash “slapped cheek” appearance
Rubella like rash: maculopapular rash
Arthralgia or arthritis
Chronic anaemia in pregnant women who are immunocompromised
Foetal clinical manifestations
Spontaneous miscarriage, stillbirth
Hydrops fetalis: Abnormal build-up of fluid in foetal tissues and organs causing oedema. 2-17 weeks after maternal infection
Investigations
Management
If both IgG and IgM positive (indicates recent infection):
Monitor with serial fetal ultrasound and middle cerebral artery Doppler
Rubella
Overview: congenital rubella syndrome is a condition which affects a foetus whilst in utero in a mother infected by rubella virus. It is the most dangerous if infection occurs in the first 12 weeks of pregnancy.17 Organism: Rubella virusTransmission 19
Droplet spread or direct contact with nasopharyngeal secretions
Vertical transmission from mother to foetusCommunicable period: 1 week before to 4 days after the onset of the rash. Most infectious when rash is erupting
Maternal clinical manifestations 19
Initially, a low grade fever
Then, maculopapular rash of cephalocaudal spread (head → downwards)
Post-auricular lymphadenopathy
Poly-arthritis
conjunctivitis
miscarriage
Foetal/neonatal clinical manifestations 20
TRIAD: deafness, cataracts, congenital heart disease
Congenital heart disease includes: PDA, pulmonary artery stenosis, ventricular septal defect, atrial septal defect
Intellectual disability
Hepatosplenomegaly
Low birth weight
“blueberry muffin” rash
stillbirth
Investigations 17
Rubella virus IgG and IgM: done at first appointment for all pregnant mothers “booking bloods”
If requiring prenatal foetal diagnosis : NAAT on amniotic fluid, foetal blood or chorionic villus biopsies
If requiring post-natal foetal diagnosis: IgG antibodies ELISA for rubella virus
Management 17
If <18 weeks, may consider counselling on termination of pregnancy
May try normal human immunoglobulin (NHIG) as post-exposure prophylaxis within 5 days of infection → does not eliminate, but reduces risk of rubella
Prevention
MMR vaccine at least 4 weeks before pregnancy if never had before
Cytomegalovirus21
Overview: CMV is part of the herpes virus familyOrganism: cyotmegalovirusTransmission 22 : contact with the saliva, nasal mucous, urine, breast milk, semen and vaginal secretions of those who are infectedMaternal clinical manifestations
Mostly asymptomatic
May have fever, lymphadenopathy, sore throat
Foetal/neonatal clinical manifestations
Petechiae
Deafness
Intellectual impairment
Pneumonitis
Blindness, chorioretinitis
Microcephaly
seizures
Investigations 21
Serology: IgG and IgM
PCR testing on blood, urine, saliva → not first line investigation
If mother positive, in utero:
Foetal ultrasound: foetal ascites, hepatomegaly, IGR, pleural or pericardial effusion , abdominal calcifications, microcephaly, oligo or polyhydramnios, hydrocephalus, intracranial calcifications
May need amniocentesis for PCR
After born:
Serology: CMV igM
CMV PCR: urine, saliva or blood
Ophthalmology review
Head ultrasound or MRI : periventricular calcification, ventriculomegaly, cerebral atrophy, white matter abnormalities
Management 21
Management may include the following
Consult obstetrics/gyane and paeditrician
Anti-virals
CMV hyperimmune globulin
Counselling and consideration of termination of pregnancy
Prevention 22 :
Wash hands thoroughly after contact with young children, changing nappies
Avoid contact with bodily fluids of young children: e.g., sharing food, drinks, kissing
CMV is the most common congenital viral infection and may be asymptomatic in the mother.
Herpes simplex virus23
Overview : Neonatal herpes simplex virus infections are rare but can cause significant morbidity and mortality . Organism : HSV 1 or 2. Primarily HSV2Transmission
HSV1: Contact with infected sores, saliva or skin surfaces in or around the mouth
HSV2: sex through contact with genital or anal surfaces, skin, sores or fluids that are infected
Maternal clinical manifestations
Usually asymptomatic
May have vesicular sores in the genital region
Foetal/Neonatal clinical manifestations: occur anywhere between birth and 6 weeks of age
Fever
Vesicular rash
Hypo or hyperpigmentation of skin
Eye: retinal dysplasia, optic atrophy, chorioretinitis
Neurological: microcephaly, encephalomalacia, intracranial calcifications
seizures
Disseminated infection: features of sepsis , negative cultures, severe liver dysfunction, consumptive coagulopathy within 30 days of life
Investigations
HSV PCR typing from genital tract of mother
Post-partum if asymptomatic and high risk of HSV infection
Swab of neonates eye, throat, umbilicus and rectum for PCR
Urine for PCR
FBC
LFTs
Coagulation profile
Postpartum if clinical signs of HSV are present
Management 24
First and second trimester acquisition of HSV
Suppression with anti-virals at 36 weeks:
acyclovir 400mg 3x daily until birth, OR
valaciclovir 500mg 2x daily until birth
vaginal birth should be anticipated
third trimester acquisition
acyclovir 400mg 3x daily until birth, OR
valaciclovir 500mg 2x daily until birth
Caesarean section should be anticipated. If rupture of membranes occur, delivery should be within 4 hours preferably.
For the neonate :
if asymptomatic and high risk of infection: HSV infection close to birth or baby born through birth canal with active maternal HSV infection, and no previous history of genital HSV
Intravenous acyclovir 10 days
If symptomatic: intravenous acyclovir
If confined to skin, eye and mouth: 14 days
For encephalitis or disseminated disease: 21 days
Prevention
Advising abstinence or use of barrier contraception during pregnancy if one partner has a history of genital herpes
Group B Streptococcus (GBS) infection in pregnancy25
Overview: GBS is a bacteria found in the vagina and bowel in 10-30% of all women. Pregnant women who carry GBS can pass it onto the neonate in the intrapartum period which can cause significant complications in the newborn. Organism: Group B StreptococcusTransmission: intrapartum Risk factors for GBS infection in mother
Preterm labourRupture of membranes >18 hours prior to birth
GBS colonisation in current pregnancy
Previous baby with GBS disease
Maternal clinical manifestations
Chorioamnionitis
Urinary tract infection
endometritis
Foetal clinical manifestations
Difficulty breathing, tachypnoea , noisy breathing, fever, difficulty feeding, cyanosis , irritability
Complications: pneumonia , sepsis, meningitis
Investigations
High vaginal swab for GBS for all women at 25-27 weeks
Management 25
if term premature rupture of membranes (PROM) and:
positive: recommend induction of labour (IOL) and intrapartum antibiotic prophylaxis (IAP) (as per below)
negative: offer IOL
if risk factors for GBS infection: give IAP
if preterm PROM
recommend IAP regardless of GBS status
intrapartum antibiotic prophylaxis:
benzylpenicillin 3g IV as a loading dose at onset of labour
benzylpenicillin 1.8g IV every 4 hours until birth
for neonate
if signs of neonatal infection, clinical chorioamnionitis consider IAP
benzylpenicillin OR ampicillin/amoxicillin AND gentamicin
Chorioamnionitis26
Overview:
chorioamnionitis refers to an infection of the placental tissues and amniotic fluid. It can occur antepartum, intrapartum or postpartum.
Organisms : polymicrobial
Caused by ascending cervicovaginal organisms
E.g., GBS, enterobacteria, mycoplasmas
Transmission: ascending infection from the lower genital tractMaternal clinical manifestations
Fever (38 or more) and ruptured membranes
Fever during labour
Uterine tenderness
Purulent amniotic fluid
Complications: PPH due to atony
Foetal clinical manifestations
Investigations
Blood cultures if ≥ 38°CLow vaginal swab culture
Mid stream urine culture
Placenta culture
Management 26
Amoxicillin 2g IV 6 hourly OR Cefazolin 2g IV 8 hourly
AND gentamicin AND Metronidazole 500mg IV 12 hourly
References
Boucoiran I, Kakkar F, Renaud C. Maternal infections. Handb Clin Neurol . 2020;173:401-422. doi: 10.1016/B978-0-444-64150-2.00029-0.
Maurice A, Tesini BL. Congenital Toxoplasmosis. MSD Manuals: Professional Version. Merck and Co; 2025. Accessed June 23, 2025. https://www.msdmanuals.com/professional/pediatrics/infections-in-neonates/congenital-toxoplasmosis
Department of Health. Toxoplasmosis. Infectious Diseases: Guidelines and Advice. Victorian Government; 2015. Accessed June 23, 2025. https://www.health.vic.gov.au/infectious-diseases/toxoplasmosis
SA Maternal & Neonatal Clinical Network. Toxoplasmosis in Pregnancy. South Australian Perinatal Practice Guidelines, Government of South Australia; 2018. Accessed June 14, 2025. https://www.sahealth.sa.gov.au/wps/wcm/connect/b82392004eedfb8fb7c2b76a7ac0d6e4/Toxoplasmosis+in+pregnancy_July2015.pdf?MOD=AJPERES&CACHEID=b82392004eedfb8fb7c2b76a7ac0d6e4
Queensland Clinical Guidelines. Syphilis and Pregnancy, Queensland Government; 2024. Accessed June 14, 2025. https://www.health.qld.gov.au/__data/assets/pdf_file/0035/736883/g-sip.pdf
Department of Health. Congenital Syphilis. Infectious Diseases: Guidelines and Advice. Victorian Government; 2022. Accessed June 15, 2025.
SA Maternal & Neonatal Clinical Network. HIV in Pregnancy. South Australian Perinatal Practice Guidelines, Government of South Australia; 2018. Accessed June 14, 2025. https://www.sahealth.sa.gov.au/wps/wcm/connect/72e4fb004ee48cd282518fd150ce4f37/HIV+in+Pregnancy_July2015.pdf?MOD=AJPERES&CACHEID=72e4fb004ee48cd282518fd150ce4f37#:~:text=%3E%20Cervical%20cytology%20(unless%20a%20recorded,within%20the%20last%2012%20months).&text=%3E%20HIV%20screening%20is%20offered%20to,with%20the%20option%20to%20decline .
Irshad U, Mahdy H, Tonismae T. HIV in Pregnancy. Treasure Island (FL): StatPearls Publishing; 2023.
Arikan Y, Burdge DR. Human immunodeficiency virus infection in pregnancy. Can J Infect Dis . 1998 Sep;9(5):301-9. doi: 10.1155/1998/274694.
SA Maternal & Neonatal Clinical Network. Hepatitis B in Pregnancy. South Australian Perinatal Practice Guidelines, Government of South Australia; 2025. Accessed June 14, 2025. https://www.sahealth.sa.gov.au/wps/wcm/connect/b8cae3804ee484c881678dd150ce4f37/Hepatitis+B+in+Pregnancy_v6_0.pdf
Asafo-Agyei KO, Samant H. Pregnancy and Viral Hepatitis. Treasure Island (FL): StatPearls Publishing; 2025.
Maurice A. Hepatitis B Virus (HBV) Infection in Newborns. MSD Manuals: Professional Version. Merck and Co; 2025. Accessed June 18, 2025. https://www.msdmanuals.com/home/children-s-health-issues/infections-in-newborns/hepatitis-b-virus-hbv-infection-in-newborns
Royal College of Obstetricians and Gynaecologists. Chickenpox in Pregnancy. RCOG;2018. Accessed June 15, 2025. https://ranzcog.edu.au/wp-content/uploads/RCOG-Chickenpox-in-Pregnancy.pdf
Bhavsar SM, Mangat C. Congenital Varicella Syndrome. Treasure Island (FL): StatPearls Publishing; 2023.
SA Maternal & Neonatal Clinical Network. Varicella Zoster (chicken pox) in Pregnnacy Clinical Guideline. South Australian Perinatal Practice Guidelines, Government of South Australia; 2018. Accessed June 14, 2025. https://www.sahealth.sa.gov.au/wps/wcm/connect/a69e3d004eee7fab80d3a36a7ac0d6e4/Varicella+Zoster+Chicken+Pox+in+Pregnancy_Sept2015.pdf?MOD=AJPERES
SA Maternal & Neonatal Clinical Network. Parvovirus in Pregnnacy Clinical Guideline. South Australian Perinatal Practice Guidelines, Government of South Australia; 2021. Accessed June 14, 2025. https://www.sahealth.sa.gov.au/wps/wcm/connect/04ab65004ee541dda794afd150ce4f37/Parvovirus+in+Pregnancy_PPG_v5_1.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-04ab65004ee541dda794afd150ce4f37-p4cj6no
Centers for Disease Control and Prevention. Pregnancy and rubella [Internet}. United States of America: US Department of Health and Human Services; 2024 [cited 2025 June 16]. Available from: https://www.cdc.gov/rubella/pregnancy/index.html
Queensland Health. Rubella [Internet]. Queensland, Australia: Queensland Government; 2023 [cited 2025 June 16]. Available from: https://www.health.qld.gov.au/cdcg/index/rubella
Medu O, Mahajan P, Hennink M, Stang L, Anderson M, Tan B, Oyenubi A, Plamondon M, Salvadori MI, Franklin K, Primeau C, Hiebert J, Minion J, Diener T. Congenital rubella syndrome, a case series. Can Commun Dis Rep . 2024;50(7-8):274-281. doi: 10.14745/ccdr.v50i78a05
Shukla S, Maraqa NF. Congenital Rubella. Treasure Island (FL): StatPearls Publishing; 2023.
Department for Health and Wellbeing, South Australia. Cytomegalovirus. Clinical Guideline. South Australian Perinatal Practice Guidelines, Government of South Australia; 2022. Accessed June 14, 2025
NSW Health. Cytomegalovirus (CMV) and Pregnancy Fact Sheet [Internet]. Australia: NSW Government; 2017 [cited 2025 June 15]. Available from: https://www.health.nsw.gov.au/Infectious/factsheets/Pages/cmv-and-pregnancy.aspx
Fernandes ND, Arya K, Syed HA, et al. Congenital Herpes Simplex. Treasure Island (FL): StatPearls Publishing; 2024.
Department for Health and Wellbeing, Government of South Australia. Genital Herpes Simplex (HSV) Infection in Pregnancy. South Australian Perinatal Practice Guidelines, Government of South Australia; 2022. Accessed June 14, 2025. https://www.sahealth.sa.gov.au/wps/wcm/connect/04ab65004ee541dda794afd150ce4f37/Parvovirus+in+Pregnancy_PPG_v5_1.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-04ab65004ee541dda794afd150ce4f37-p4cj6no
Queensland Clinical Guidelines. Early Onset Group B Streptococcal Disease (EOGBSD), Queensland Government; 2025. Accessed June 14, 2025.
Government of Western Australia North Metropolitan Health Service. Infections in Obstretrics (Intra-amniotic Chorioamnionitis And Postpartum Infection): Diagnosis and Management, Government of Western Australia; 2024. Accessed Jun 20, 2025.











Discussion