Personality Disorders

“I’m so good at beginnings, but in the end I always seem to destroy everything, including myself.”
― Kiera Van Gelder
“I need them to be aware and present with me in the midst of the storm, not just tell me what to do.”
― Kiera Van Gelder
The term ‘personality disorder’ is frequently used in clinical practice to describe individuals with pervasive difficulties in interpersonal functioning, self-concept, emotional regulation and behaviour. Difficulties in personality functioning are potentially disabling conditions and are associated with significant distress and interpersonal difficulties.
Effects of personality
Characteristics of a “successful” personality
Personality: pattern of perceiving, relating and beliefs about oneself and the environment as it is exhibited in actions in social, interpersonal and intrapersonal contexts
Personality Disorder: Pattern of inner experience and behaviours not consistent with culture in two of the following:
Cognition ( unusual ways of analysis of self, other, or events)
Affect (range, intensity, lability and appropriateness)
Interpersonal functioning Impulse control
Interview
History
Types of Personality Disorders
| PERSONALITY DISORDER CLUSTERS | ||
| Cluster | Subtype | Key features |
| A. Odd/eccentric (MAD) | Paranoid | Suspcious |
| Schizoid | Sociall indifferent | |
| Schizotypal | Eccentric | |
| B. Dramatic/emotional (BAD) | Antisocial | Unempathic, callous |
| Borderline | Unstable identity | |
| Hisrionic | Attention-seeking | |
| Narcissisic | Self-centred, grandiose | |
| C. Anxious/fearful (SAD) | Avoidant | Inhibited |
| Dependent | Submissive, anxious | |
| Obsessive | Perfectionistic, rigid | |
| Classification of personality disorder | ||||
| Cluster A – Mad, Odd and eccentric | Schizoid: loner, detached, flat affect, restricted emotions | Schizotypal: odd, eccentric, magical thinking, paranoid | Paranoid: distrustful and suspicious | |
| Cluster B – Bad, dramatic and erratic | Histrionic: excessively emotional, attention-seeking | Narcissistic: self-important, needs admiration, lacks empathy | Antisocial: lacks empathy towards others. | Borderline: impulsive, unstable relationship, splitting (love then hate), attentionseeking |
| Cluster C Sad, anxious and timid | Obsessive-compulsive | Avoidant, Hypersensitive to criticism, socially uncomfortable, seeks out interpersonal relationships but with great discomfort | Dependent: submissive,clinging, needs to be taken care of | |
Persistence and pervasiveness is required in all the above criteria.
| Risk assessment in personality disorder |
| History of suicidal and self-harming behaviours and feelings |
| Triggers for self-harming behaviour |
| Degree of planning and intent |
| Chronic versus acute suicidal ideation |
| Available interpersonal support and responses elicited from carers/supports |
| Past intervention strategies and capacity to engage |
Self-harm/ self-injury: Refers to people deliberately hurting their bodies and is often done in secret without anyone else knowing.
General criteria for personality disorder
The essential features of a personality disorder are
Most common and most common to present is borderline personality Disorder. Borderline personality disorder is a severe mental disorder that has its onset during adolescence and emerging adulthood. It affects up to 3% of the population and occurs almost equally among males and females. Borderline personality disorder is Cluster B.
Borderline personality disorder is a severe mental disorder that has its onset during adolescence and emerging adulthood. It affects up to 3% of the population. Borderline personality disorder are thought to result from the impact of trauma and neglect in early development on vulnerable individuals.
Borderline personality disorder is characterised by a pervasive pattern of instability in emotional regulation, interpersonal relationships and self-image, along with marked impulsivity.
Course of Borderline Personality Disorder
Drugs should not be used as primary therapy for borderline personality disorder, because they have only modest and inconsistent effects, and do not change the nature and course of the disorder.
Dialectical Behavioral Therapy Integration of CBT with mindfulness, acceptance and techniques to tolerate stress and control emotions. It teaches skills to control intense emotions, reduce self-destructive behaviours and improve relationships. Four skill that are taught in DBT: 1. Mindfulness, Distress tolerance, interpersonal effectiveness and emotional regulation.
Remember there are many types of personality disorder all with distinct features.
| PERSONALITY DISORDER CLUSTERS | ||
| Cluster | Subtype | Key features |
| A. Odd/eccentric (MAD) | Paranoid | Suspcious |
| Schizoid | Sociall indifferent | |
| Schizotypal | Eccentric | |
| B. Dramatic/emotional (BAD) | Antisocial | Unempathic, callous |
| Borderline | Unstable identity | |
| Hisrionic | Attention-seeking | |
| Narcissisic | Self-centred, grandiose | |
| C. Anxious/fearful (SAD) | Avoidant | Inhibited |
| Dependent | Submissive, anxious | |
| Obsessive | Perfectionistic, rigid | |
General principles of management include consistency, reliability, encouraging autonomy, and the sensitive management of change
Non-pharmacological Management
Pharmacological Management (short-term)
| PERSONALITY DISORDER CLUSTERS | |||
| Cluster | Subtype | Therapy | Medication (usually short-term) |
| A. Odd/eccentric (MAD) | Paranoid | Reluctant to seek help. Referral for substance abuse if necessary | Low-dose antipsychotics |
| Schizoid | Low-dose antipsychotics | ||
| Schizotypal | Low-dose antipsychotics | ||
| B. Dramatic/emotional (BAD) | Antisocial | Contingency management treatment (a behavioural therapy where adaptive behaviours are rewarded | |
| Borderline | Alot discussed more at the borderline personality disorder section | ||
| Hisrionic | |||
| Narcissisic | |||
| C. Anxious/fearful (SAD) | Avoidant | CBT | |
| Dependent | Cognitive behavioural, psychodynamic, and social skills training, substance abuse therapy | ||
| Obsessive | Cognitive behavioural, psychodynamic, and social skills training, substance abuse therapy | ||
Consequences of personality disorders
All clusters worse under stress, especially interpersonal.
Depression, anxiety, substance use, suicidal behaviour, and suicide are all more common in these patients; comorbid mental health problems are more difficult to treat and have poorer outcomes.
Suicide is widespread across many age groups, and is associated with mental illness such as depression and other factors. Suicide is likely to be under-reported as deaths from suicide may be difficult to distinguish from accidental or intentional injury. It is important to note that suicide attempts are up to 20 times more frequent than completed suicide.
Suicide among medical practitioners is higher than other professional groups in many industrialised countries, especially among female doctors. Risk factors for suicide are the same as the general population, however there is greater knowledge about how succeed and the availability of methods which may contribute to relatively high suicide rates.
Mental illness: A term referring to a group of conditions that significant affect how a person feels, thinks, behaves, and interacts.
Mentally disordered person: A person (whether or not suffering from mental illness) whose behavior for the time being is so irrational as to justify a conclusion on reasonable grounds that temporary care, treatment, or control of the person is necessary.
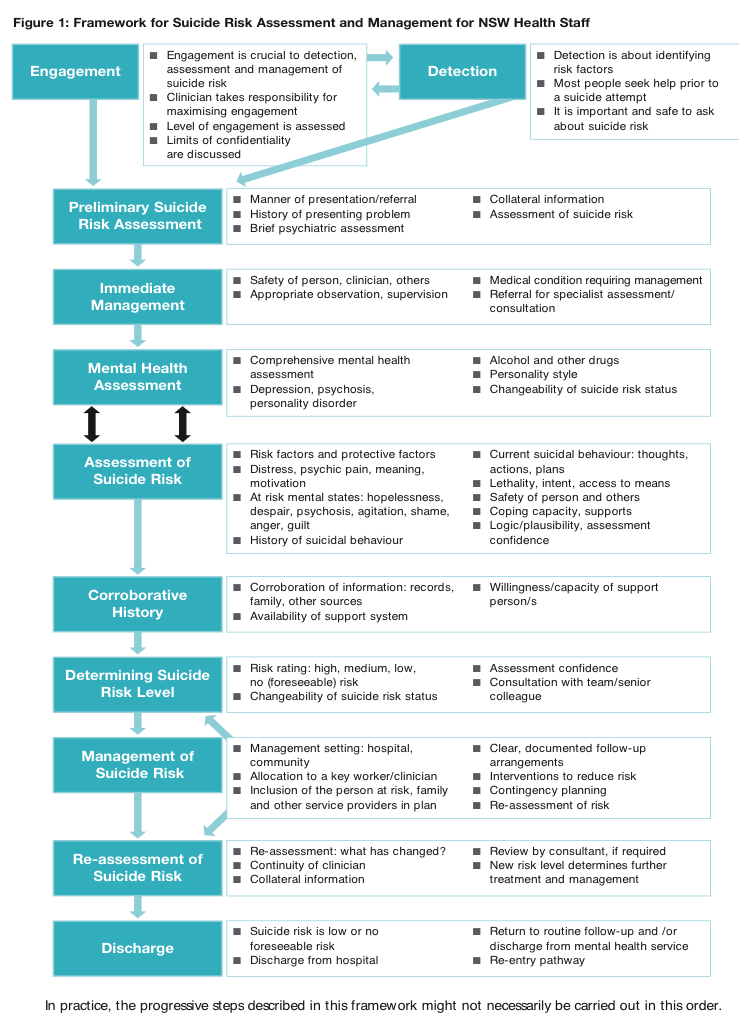
Suicide risk assessment – Important to complete when dealing with all patients who have mental health problems. The aim is to evaluate the likelihood of suicide attempt in the period of assessment.
Self-harm assessment (brief)
| RISK FACTORS AND PROTECTIVE FACTORS OF SUICIDE | ||
| Groups at Risk of suicide | Risk Factors | Protective Factors |
| History of attempt or self-harm | Male | Strong perceived social supports |
| History of mental illness | Between 25-44yo | Family cohesion |
| History of sexual or physical abuse/neglect | Older people | Peer group affiliation |
| Domestic violence | Living in rural areas | Good coping and problem solving skills |
| Substance abuse | Recent break-up | Positive values and beliefs |
| Physical illness | Sexual identity conflicts | Ability to seek and access help |
| Refugees, immigrants | Financial difficulties | |
| Homeless | Impending legal prosecutions | |
| Lack of support |
Involuntary treatment
Discharge following admission
Chanen, AM., Thompson, KN. (2016). Prescribing and borderline personality disorder. Australian Prescirber. 39(2). 49-53.












Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion