Acute Respiratory Failure


Acute Respiratory failure causes hypoxia and/or impaired ventilation with hypercapnia, leading to severe hypoxemia and rapid deterioration. Two main types of respiratory failure:
Confirm diagnosis of respiratory failure with ABG.
Acute Respiratory Failure:
Acute Respiratory Failure Type I: Hypoxaemia (PaO2<60mmHg) without hypercapnia. Caused by conditions affecting oxygenation: right-to-left shunts or V/Q mismatch
Acute Respiratory Failure Type II:
Chronic Respiratory Failure
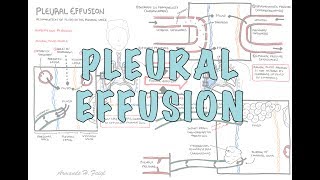
Acute Respiratory Distress Syndrome: an acute, diffuse, inflammatory lung injury that leads to increased pulmonary vascular permeability, increased lung weight, and a loss of aerated tissue.
| CAUSES OF ACURE RESPIRATORY FAILURE | |
| Type I | Type II |
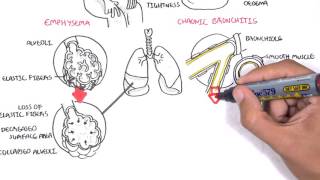
| Pneumonia | COPD |
| ARDS | Life-threatening asthma |
| Interstitial lung Disease | Drug Intoxication (opioids) |
| Acute Pulmonary Oedema | CVA/trauma |
| Asthma | Primary muscles disorders |
| COPD | Myasthenia gravis |
| Pneumothorax | Poliomyelititis |
| Pulmonary Embolism | Kyphoscoliosis |
| Obesity | Polyneuropathies |
| Pulmonary hypertension | Obesity |
Clinical Presentation
Increased work of breathing
Signs of Hypoxia
Hypoventilation
Obstruction
Use pulse oximetry, ECG, ABG and Chest X-ray in the initial assessment.
Check pupils to check for opioid use or other drugs causing respiratory depressants.
Continuously check changes in ABG throughout management.
Ongoing Management If CO2 still increasing or O2 saturation is not improving (>88%) in order:
Identify and treat underlying cause!
Positive pressure invasive mechanical ventilation will decrease cardiac output due to decreased venous return.
Overview
Hypoxaemia (PaO2<60mmHg) without hypercapnia. Caused by conditions affecting oxygenation: right-to-left shunts or V/Q mismatch.
| CAUSES OF ACURE RESPIRATORY FAILURE | |
| Type I | Type II |
| Pneumonia | COPD |
| ARDS | Severe Asthma |
| Interstitial lung Disease | Drug Intoxication (opioids) |
| Acute Pulmonary Oedema | CVA/trauma |
| Asthma | Primary muscles disorders |
| COPD | Myasthenia gravis |
| Pneumothorax | Poliomyelititis |
| Pulmonary Embolism | Kyphoscoliosis |
| Obesity | Polyneuropathies |
| Pulmonary hypertension | Obesity |
Management

Overview
Hypoxaemia with hypercapnia (PaCO2>50mmHg).
Clinical Presentation
Pathophysiology – Hypercapnia when alveolar ventilation insufficient to excrete volume of CO2 produced by tissue metabolism due to:
Aims of treatment here is to achieving safe oxygen concentration without increasing CO2 and acidosis, while identifying precipitating condition.
Becareful using oxygen in COPD. Severe COPD hypoventilate and retain CO2. Giving uncontrolled O2 may increase CO2.
Overview
ARDS is an acute, diffuse, inflammatory lung injury that leads to increased pulmonary vascular permeability, increased lung weight, and a loss of aerated tissue. Clinical hallmarks of ARDS are hypoxemia and bilateral radiographic opacities, while the pathological hallmark is diffuse alveolar damage.
More Information on Acute Respiratory Distress Syndrome
Overview
| Indications for lung transplantation |
| Severe COPD |
| Cystic fibrosis |
| Bronchiectasis |
| Progressive Interstitial lung disease |
| Pulmonary hypertension |
| Eisenmenger’s syndrome |
Contraindications
Relative
Absolute
Intermittant Mandatory Ventilation: Patient Paralysed/Sedation [No spontaneous effort]
Volume Control Ventilation
Pressure Control Ventilation

















Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion