

Asthma
Overview
Asthma is a chronic airway inflammation disorder due to complex interactions between inflammatory cells, mediators and airway cells. In young children in whom lung function testing is not feasible, including most preschool children, asthma is defined by the presence of variable respiratory symptoms. Asthma is one of the most common causes of presentation to the Emergency department It implies reversible airway constriction (peak flows vary by >20%) +/- wheeze, dyspnoea or cough.
Definition
Asthma: Condition of bronchial hyperactivity and smooth muscle hypertrophy leading to a chronic inflammatory condition of the airways associated with widespread bronchospasm that is reversible.
Acute cough: Condition for less than 3 weeks, most commonly caused by acute upper respiratory infection but also may be caused by congestive heart failure, pneumonia, and pulmonary embolism.
Chronic cough: Condition for longer than 3 to 8 weeks (case definitions vary). Smoker – chronic obstructive pulmonary disease. Nonsmoker with a normal chest radiograph and not taking an ACE inhibitor, it may be due to postnasal drip, gastroesophageal reflux disease (GERD), or asthma.
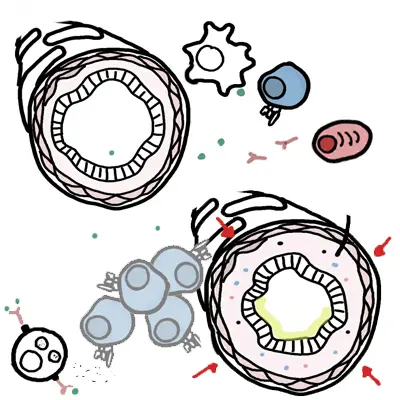
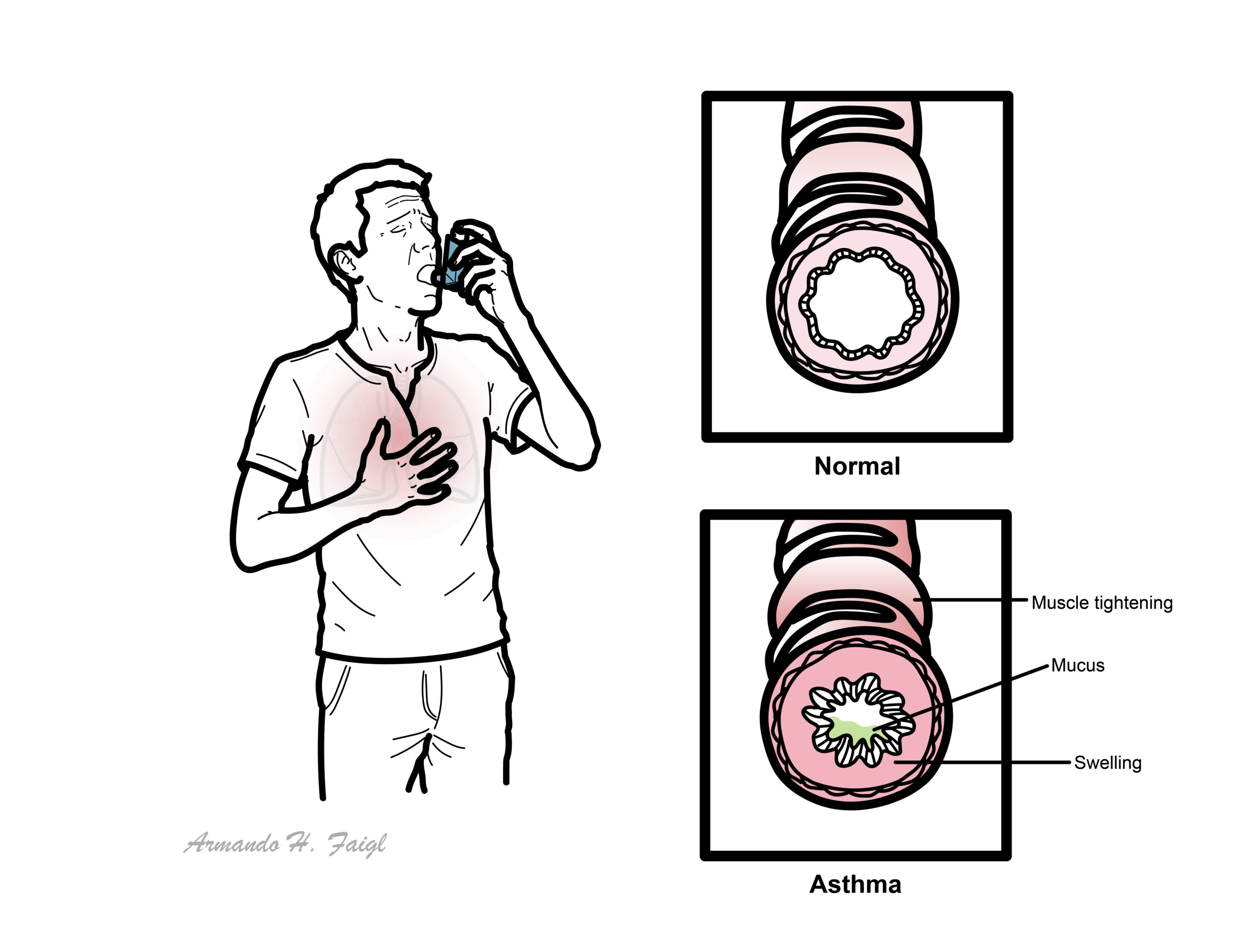
Airway obstruction occurs due to a combination of:
- Inflammatory cell infiltration
- Mucus hypersecretion with mucus plug formation
- Smooth muscle contraction
This page will mainly focus on paediatric asthma
Epidemiology
- Paediatric asthma is the most common chronic respiratory disease in the developed world, with the highest prevalence found in English-speaking countries such as the US, the UK, and Australia.
- Good control of asthma and prevention of exacerbations is important.
- There is a variable gender effect, with a higher prevalence in prepubertal males and postpubertal females
- Between 30-80% of children become asymptomatic around the time of puberty.
Patterns of Asthma
Infrequent intermittent asthma (70-75% of cases)
- Episodes of asthma lasting days to a week
- Episodes are generally 6 or more weeks apart
- Asthma triggered my URTI
- No need for preventer
Frequent intermittent asthma (20-25% of cases)
- Episodes occur at intervals less than 6 weeks
- Minimal symptoms between episodes
- Children may benefit from regular preventative therapy usually with ICS or Leukotriene antagonist
Persistent asthma (5-10% of cases)
- Symptoms on most days including:
- Disruption of sleep due to wheeze and cough
- Early morning dyspnoea
- Exercise dyspnoea or activity intolerance
- Require preventive therapy
- Referral to a paediatrician
Aetiology and Risk Factors
Aetiology
- Genetic predisposition
- Triggers
- Infections à viral (up to 80% of hospital admissions for asthma are following a viral illness)
- Exercise (especially in dry, cold air)
- Allergens (dust mites, pollen, food, animal dander)
- Environment smoking
- Chemicals (salicylates)
- Allergic sensitisation
- Atopy
- Family History
- Passive or Active tobacoo smoker
- Viral infections
- Higher serum eosinophils
Pathophysiology
Clinical Manifestation
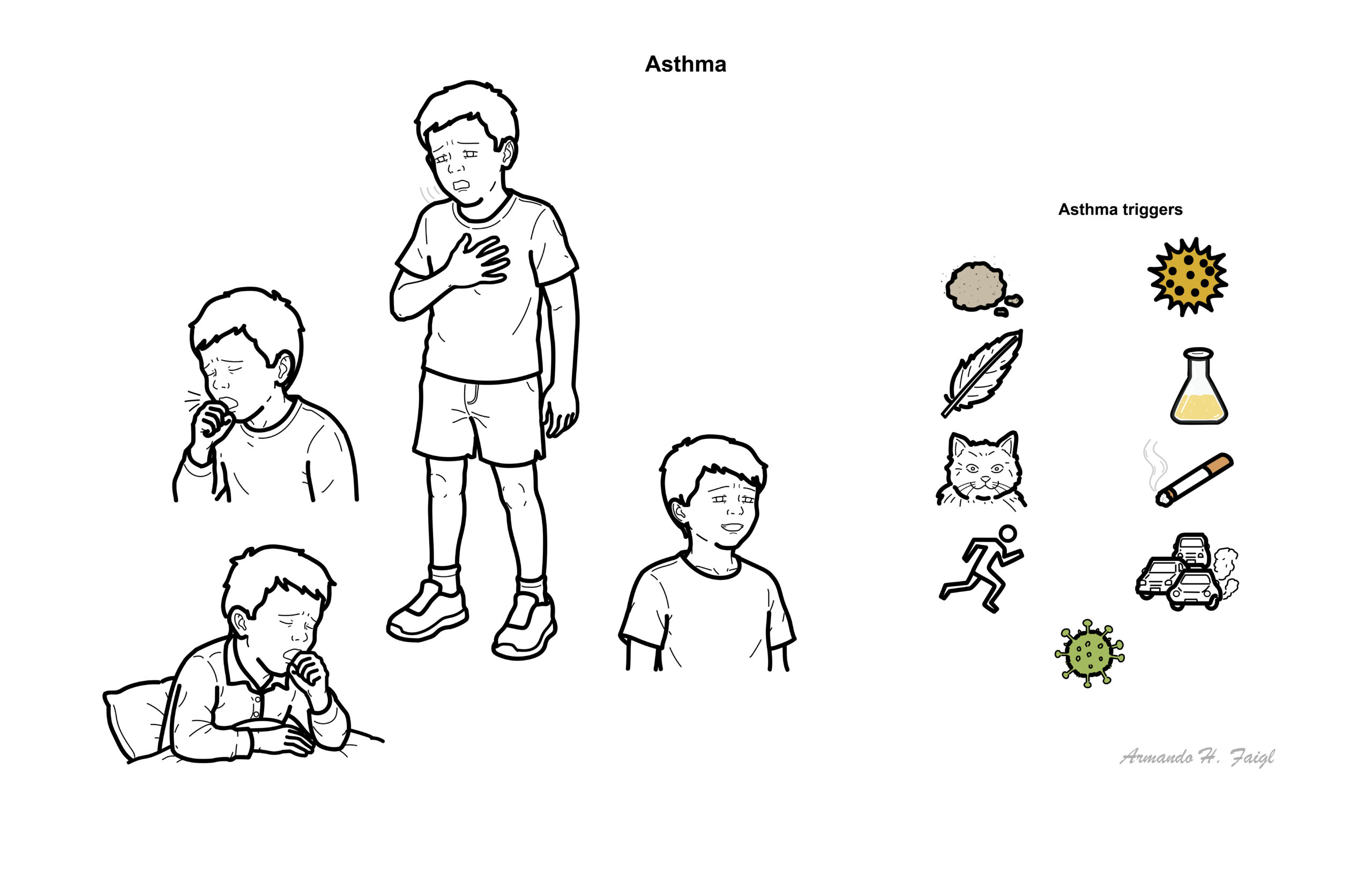
Typical features
- Recurrent wheeze
- Cough, especially:
- At night or early morning
- During or after exercise
- With laughter or crying
- During viral infections
- Shortness of breath
- Chest tightness
- Reduced exercise tolerance
- Night waking
- Symptoms varying between days or seasons
- Prolonged cough or wheeze after respiratory infections
Clinical Examination
Examination may be normal between episodes.
During symptomatic periods:
- Expiratory wheeze
- Prolonged expiration
- Tachypnoea
- Increased work of breathing
- Intercostal or subcostal recession
- Tracheal tug
- Reduced air entry
- Hyperinflated chest in longstanding severe disease
A quiet or silent chest in a distressed child indicates critically reduced airflow rather than improvement.
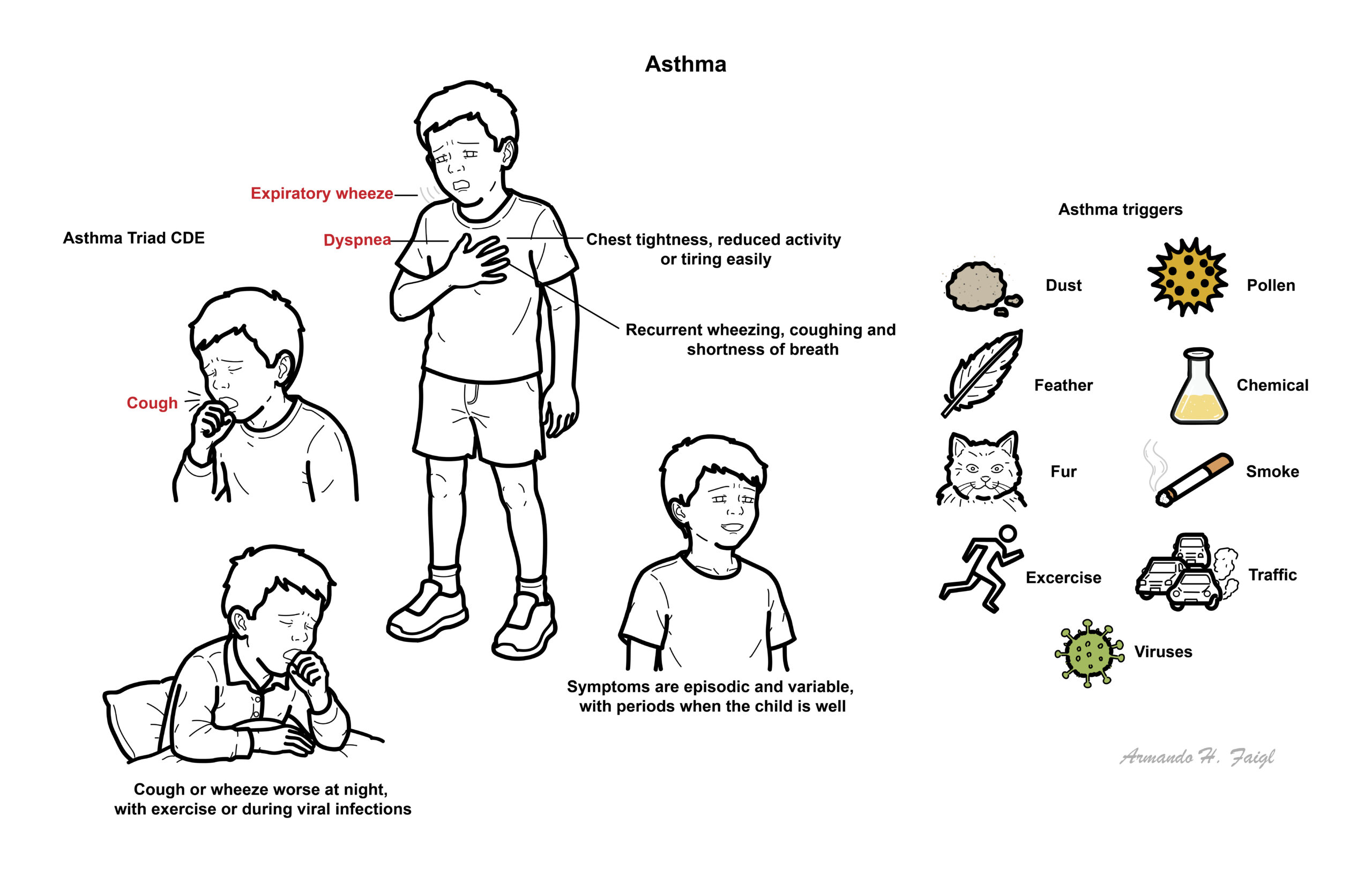
Asthma Triad CDE: Cough, Dyspnea, Expiratory wheeze
A silent chest, exhaustion or altered consciousness indicates life-threatening asthma.
Features of severe or life-threatening asthma
- Unable to speak in full sentences, drink or feed
- Marked recession or respiratory distress
- Agitation, exhaustion, confusion or drowsiness
- Cyanosis
- Poor respiratory effort
- Markedly reduced air entry or silent chest
- Oxygen desaturation
- Bradycardia or respiratory arrest
Parental anxiety should not be discounted: it is often of significance even if the child appears relatively well.
Certain thing can trigger a wheezing episode in asthma
- Pollen
- Dust
- Featheres
- Fur
- Excercise,
- Viruses
- Chemical
- Smoke
- Traffic
Diagnosis
Diagnosis requires:
- A history of variable respiratory symptoms suggestive of asthma.
- Objective evidence of variable expiratory airflow limitation where possible.
Spirometry with bronchodilator responsiveness is the preferred initial objective test:
- Measure FEV₁, FVC and FEV₁/FVC before bronchodilator.
- Repeat 10–15 minutes after salbutamol.
- An increase in FEV₁ greater than 10% of the predicted FEV₁ supports asthma in children.
- Normal spirometry when asymptomatic does not exclude asthma, and testing may need to be repeated during symptoms.
Other supportive tests include:
- Fractional exhaled nitric oxide—FeNO
- Peak expiratory flow monitoring
- Exercise or bronchial-challenge testing
- Blood eosinophils
- Allergy testing where clinically relevant
FeNO and eosinophils may support type 2 inflammation but do not independently diagnose or exclude asthma. Previous inhaled corticosteroid treatment can normalise these tests.
Children aged 1–5 years
Objective lung-function testing is often not feasible. Diagnosis is based on clinical history
Consider an 8–12-week trial of low-dose inhaled corticosteroid plus salbutamol as needed. Significant improvement during treatment, followed by recurrence after withdrawal, supports preschool asthma.
- Foreign Body
- Pertussis
- Croup
- Pneumonia/TB (Do X-Ray!)
- Aspiration
- Cystic Fibrosis
- Transient infant wheezing
- Sinusitis
- Cardiac failure due to congenital heart disease
- Structural airway abnormality – laryngomalacia, vascular ring
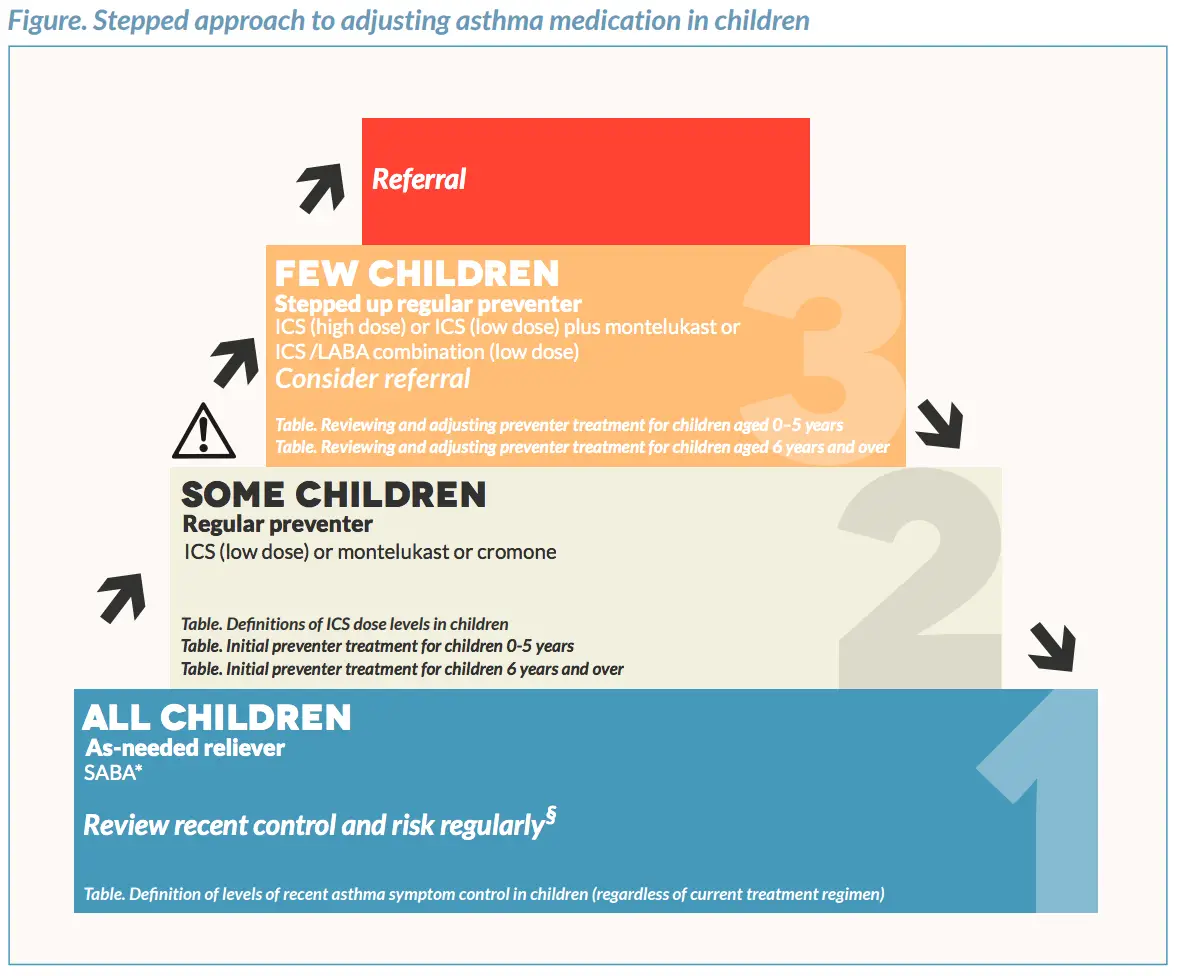
Treatment
General management
- Educate the child, parents, carers and school staff.
- Provide a written, personalised asthma action plan.
- Check inhaler technique and adherence at every review.
- Use a pressurised metered-dose inhaler with a spacer; add a mask for children unable to seal their lips around the mouthpiece.
- Avoid tobacco smoke and vaping exposure.
- Encourage normal physical activity and participation in sport.
- Treat allergic rhinitis, obesity and other comorbidities.
- Identify clinically relevant triggers without imposing unnecessary allergen restrictions.
- Review asthma control, reliever use, night waking, school absence and exacerbations regularly.
Level 1
- Salbutamol as needed may be considered only for children with mild, infrequent symptoms, no severe exacerbation history and no major risk factors.
- Frequent salbutamol use indicates inadequate control and the need for ICS-containing treatment.
Level 2
- Maintenance low-dose ICS plus salbutamol as needed.
- Montelukast is a less-preferred alternative when ICS is declined or cannot be used.
Level 3
- Maintenance low-dose ICS–LABA, or
- Medium-dose ICS.
Level 4
- Maintenance medium-dose ICS–LABA.
Level 5
- Specialist severe-asthma management, which may include:
- High-dose ICS-based therapy
- Tiotropium
- Montelukast as add-on therapy
- Phenotype-directed biological treatment:
- Omalizumab: anti-IgE therapy for severe allergic asthma.
- Dupilumab: anti-IL-4 receptor therapy for moderate-to-severe type 2 asthma associated with raised eosinophils or FeNO.
Asthma action plan
The essential elements of asthma self-management education are:
- Written information about asthma and individualised patient details
- Self-monitoring of symptoms and/or lung function (spirometry, peak flow)
- A written asthma action plan
- Regular review by doctor, asthma educator, or nurse on medications and current asthma control, reinforcement of trigger avoidance behaviours and lifestyle changes if warranted, feedback to the patient about how well they are controlling their asthma, and how control can be improved
Asthma Emergency
Assessment of and management of Asthma in Emergency
- Acute Mild/moderate asthma
- Acute asthma
- Life-threathening asthma
Complications and Prognosis
- Acute severe asthma or status asthmaticus
- Hypoxaemic or hypercapnic respiratory failure
- Respiratory arrest and death
- Pneumothorax or pneumomediastinum, rarely
- Recurrent emergency presentations or hospital admissions
- Sleep disturbance and chronic fatigue
- Reduced exercise participation
- School absence and impaired learning
- Anxiety and reduced quality of life
- Airway remodelling and persistent airflow limitation
Treatment-related complications
- ICS:
- Oral candidiasis
- Dysphonia
- Small reduction in growth velocity, particularly with higher doses
- Salbutamol:
- Tremor
- Tachycardia
- Hypokalaemia and lactic acidosis with excessive dosing
- Montelukast:
- Neuropsychiatric adverse effects
- Most children can achieve good symptom control and participate normally in school, exercise and sport with appropriate treatment.
- Some children, particularly those with mild preschool viral-associated wheeze, experience remission as their airways grow.
- Poor control and recurrent exacerbations increase the risk of persistent airflow limitation.
- Childhood asthma deaths are uncommon but remain possible, particularly with previous severe attacks, inadequate ICS use, poor adherence, excessive reliever use or delayed emergency treatment.
References
- National Asthma Council Australia. Australian Asthma Handbook: the national guidelines for health professionals. Version 3.0. Melbourne: National Asthma Council Australia; 2025.
- Global Initiative for Asthma. Global strategy for asthma management and prevention. 2026 update. Fontana, WI: Global Initiative for Asthma; 2026.
- National Institute for Health and Care Excellence. Asthma: diagnosis, monitoring and chronic asthma management. NICE guideline NG245. London: NICE; 2024. Updated 2025.
- Gaillard EA, Kuehni CE, Turner S, et al. European Respiratory Society clinical practice guidelines for the diagnosis of asthma in children aged 5–16 years. Eur Respir J. 2021;58(5):2004173.
- Bacharier LB, Maspero JF, Katelaris CH, et al. Dupilumab in children with uncontrolled moderate-to-severe asthma. N Engl J Med. 2021;385(24):2230–2240.






Members only discussions coming soon…