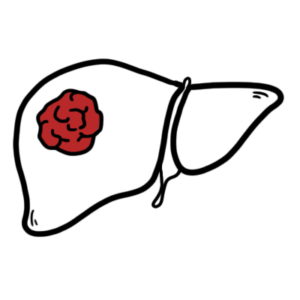
0:00 In this video, we're going to talk about acute cholisestitis. 0:07 This is an overview and introduction. 0:10 So acute cholisestitis is inflammation of the gallbladder, and it's usually 0:14 because 0:15 of obstruction of the cystic duct by gallstones. 0:19 Acute cholisestitis is the most common complication of cholilithiasis, which is 0:24 formation of gallstones 0:25 in the gallbladder. 0:27 And to be clear, cholilithiasis is formation of stones in the gallbladder, 0:32 which can lead 0:33 to a few complications, one of which is acute cholisestitis. 0:41 The other terminology, cholidocolytheasis, is formation of stones, gallstones 0:46 in the common 0:47 bile duct, but we will not focus on that here. 0:51 In this video, we will mainly focus on acute cholisestitis, but really, we will 0:56 also talk 0:57 about every other complication, and hopefully we can get our head around it 1:03 together. 1:04 So here is a guy with right upper quadrant pain of the abdomen. 1:10 Let's look at the normal anatomy of the upper GIT, partly. 1:15 So here is the gallbladder. 1:18 Now the gallbladder is an organ that stores what's called bile, and bile is a 1:23 mixture 1:24 of cholesterol and other pigments. 1:28 The bile is important in digesting fatty foods. 1:32 The bile is actually produced by the liver, and gallbladder just stores the 1:38 excess bile. 1:39 So back to the anatomy. 1:43 Here is the gallbladder, the body, the neck, and the fundus of the gallbladder. 1:52 This is the cystic duct coming out from the gallbladder and connects to the 1:57 common hepatic 1:58 ducts, which arise from the liver. 2:02 The joining of the cystic duct and common hepatic ducts forms the common bile 2:08 duct, which runs 2:09 all the way down and joins with the pancreatic duct from the pancreas. 2:16 Before moving to the pancreas, the stomach actually continues on to the small 2:21 intestine 2:21 here, transporting the half-digested food content. 2:27 The first part of the small intestine is the duodenum. 2:31 Then the duodenum goes on to the duodenum, which is the second part. 2:36 Here is the pancreatic duct I was talking about, and here is part of the pancre 2:42 as. 2:43 And essentially, the gallbladder will contract and release bile, or the liver 2:48 will release 2:49 bile, which will go down and end up in the common bile duct. 2:54 The common bile duct runs all the way down and joins with the pancreatic duct 2:59 from the 2:59 pancreas. 3:01 The newly formed duct will then release this bile and the enzymes from the panc 3:08 reas into 3:08 the duodenum through the ampula of vata to help digest food. 3:15 In acute colicistitis, a gallstone, which was formed in the gallbladder, gets 3:20 stuck in 3:21 the cystic duct. 3:23 Now a lot of us actually have gallstones in our gallbladders, but they don't 3:28 cause any 3:29 problems. 3:30 We are asymptomatic. 3:33 As people get unlucky and the gallstones get stuck either temporarily or for 3:41 some time. 3:42 There are many types of gallstones, but we won't talk about that here. 3:47 Just think of gallstones as a mixture of cholesterol and other pigments within 3:53 bile. 3:54 So when the gallstones get stuck in the cystic duct, the gallbladder will try 3:58 to contract 3:59 and push it out without any success, and this obstruction results in 4:04 inflammation to the 4:06 gallbladder, and this is acute colicistitis. 4:10 Acute colicistitis shares similar features to two other conditions, called b 4:16 iliary colic 4:17 and colonigitis. 4:19 But these three conditions do differ. 4:23 We won't talk about them now, but they differ in the pain, having fever or 4:30 increased white 4:31 cell count, and finally joined us, which is yellowing of the skin. 4:39 So what are actually these conditions? 4:42 Well biliary colic is where there is only temporary obstruction of the gall 4:47 stone at 4:48 the neck of the gallbladder, so it can go in and out. 4:54 Acute colicistitis, as we mentioned, is the gallstone stuck at the cystic duct, 4:59 causing 5:00 inflammation of the gallbladder. 5:04 And colonigitis is a complication of gallstones, where infection develops in 5:10 the common bile 5:11 duct, and this is life-threatening. 5:16 So the signs and symptoms of acute colicistitis, specifically fever, nausea, 5:24 vomiting, right 5:26 upper quadrant pain, pain which may radiate to the right side of the back. 5:34 On examination, there is a positive murphy sign. 5:38 Murphy sign is where a hand is placed at the mid inferior board of the liver. 5:44 The patient is then asked to take a deep breath in. 5:48 The diaphragm lowers during inspiration, and with our hand being placed where 5:55 it is, 5:56 it will irritate the gallbladder, as the diaphragm pushes the gallbladder down. 6:02 And this will trigger pain. 6:05 The patient becomes startled and stops breathing in. 6:11 So going back to the small table we made, the differences in the three- 6:16 conditioned biliary 6:18 colic, acute colicistitis, and colonigitis is that biliary colic only presents 6:24 with right 6:25 upper quadrant pain, typically. 6:27 Acute colicistitis, right upper quadrant pain, with fever and raised white cell 6:34 count. 6:35 And finally, colonigitis presents with right upper quadrant pain, fever, 6:40 increased white 6:40 cell count, and jaundice, yellowing of the skin. 6:44 These three findings make up what's called Charco's Triad. 6:51 Complication of colicistitis is a tumor of the gallbladder, chronic colicist 6:57 itis, mucoseal, 6:58 where mucus is secreted into the gallbladder, empaima, which is pus in the gall 7:04 bladder thanks 7:05 to infection by the bacteria. 7:08 There is Maritzi syndrome, and Maritzi syndrome is basically when the gallstone 7:13 in the cystic 7:14 duct actually impacts or obstructs the hepatic duct. 7:19 And obstruction of the hepatic duct means that the bile being produced by the 7:24 liver 7:25 will go backwards, will backflow and cause what's known as obstructive jaundice 7:31 . 7:32 Other complications include perforation of the gallbladder. 7:37 Gallbladder duodenal fistula, which allows large gallstones to pass through 7:42 causing gallstone 7:43 ilius at the terminal ileum. 7:48 Gallstones can trigger colingitis from colidocolytheasis or cholylithiasis, 7:53 when it obstructs 7:54 the common bile duct. 7:58 Gallstones can cause pancreatitis if it obstructs the passage of contents from 8:02 the pancreas 8:03 into the duodenum. 8:06 Finally obstruction at the common bile duct or above can cause backflow of bile 8:11 to the 8:11 liver. 8:13 The bile backflow can lead to obstructive jaundice. 8:20 On this side note, there is something called kavosia's law. 8:24 And kavosia's law essentially says that the presence of enlarged gallbladder 8:29 with jaundice 8:30 is unlikely due to gallstones, rather carcinoma of the head of the pancreas. 8:40 Investigations that can be performed with a person suspected of biliary tree 8:44 problems 8:45 include full blood count, which may show raised white cell counts, amylase lip 8:49 ase to 8:49 check for pancreatitis, CRP, EUCs and LFTs. 8:55 And LFTs are important because there will be abnormal LFTs with a problem that 9:01 occurs 9:01 in the biliary tree system. 9:04 Ultrasound is diagnostic and can detect gallstones and is used to elicit Murphy 9:09 's sign too. 9:11 Abdominal X-ray can only pick up 10% of gallstones. 9:17 Another imaging technique is the hider scan, which is a contrast scan that 9:21 lights up the 9:22 biliary tree. 9:23 If the biliary tree doesn't light up fully, there can be an obstruction. 9:30 The management of acute colicistitis is surgery. 9:33 Again, people can have gallstones normally. 9:36 And if they are asymptomatic, there is no reason to remove the gallbladder 9:43 unless they 9:44 have risk factors for future complications. 9:49 Surgery is done for symptomatic people or people with recurrent gallstone 9:54 disease. 9:54 The management of acute colicistitis before surgery is nil by mouth, fluids and 10:01 IV antibiotics, 10:02 pain relief with analgesia. 10:05 Surgery can be done laparoscopically or open. 10:10 Dynamic colicistectomy is done over open colicistectomy. 10:15 In laparoscopic colicistectomy, there are a few ports over holes in the abdomen 10:20 that 10:20 can be made. 10:22 These include the surgeon point under the Ziffy sternum, the Hasen camera point 10:32 , assistant 10:34 point and the accessory point. 10:39 Let us look inside the abdomen from inferior view. 10:46 The abdominal cavity is pumped with air, carbon dioxide and this makes the 10:50 surgeon's work 10:51 easier as it creates space. 10:55 So here is the liver, a gallbladder. 10:58 Here is the laparoscopic light that views the area from the Hasen camera point 11:03 and the 11:04 two assistant ports as examples of how things are assessed in the area. 11:10 So I am not a surgeon but this hopefully will give you an understanding of col 11:14 icistectomy 11:14 in general. 11:17 Firstly what happens is that they want to expose the gallbladder because the 11:22 gallbladder 11:23 and the digestive organs are surrounded by the visceral peritoneum. 11:30 When the gallbladder is exposed the cystic artery is clipped and the cystic 11:37 duct is clipped 11:38 and then incisions are made in between the clips. 11:42 This is in order to prevent spillage of contents within the ducts. 11:49 Once the incisions are made the gallbladder can be safely removed. 11:55 The cystic duct is clipped and so it doesn't bleed out. 11:59 And the cystic duct remember was clipped and so it doesn't spill anything as 12:05 well. 12:05 When the gallbladder is removed everything is put under the visceral peritoneum 12:10 once again, 12:10 it's stitched up and the surgery is done. 12:14 However, sometimes an open colicistectomy is needed. 12:19 This is especially if there are complications from the gallstones or 12:24 complications during 12:24 laparoscopic surgery in the first place. 12:28 An open colicistectomy is quicker but is much more invasive.