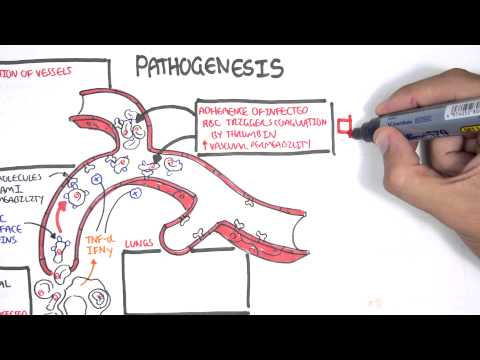
0:00 In this video, we're going to look at amebic dysentery, caused by intomibah, 0:03 histolotica, 0:06 histolotica. 0:07 I hope I pronounced that right. 0:09 So, these are the entire area. 0:12 We've got a lot of information about this, and we've got a lot of information 0:14 about that. 0:16 We've got a lot of information about this. 0:18 We've got a lot of information about this. 0:20 We've got a lot of information about this. 0:22 We've got a lot of information about this. 0:24 We've got a lot of information about this. 0:26 We've got a lot of information about this. 0:28 So, these are the intomibah histolotica, are enteric protozoaans with a 0:33 worldwide distribution. 0:36 It is stored to infect as much as 10% of the world's population. 0:41 Intomibah histolotica is a major cause of amebic dysentery. 0:47 What is amebic dysentery? 0:49 Well, there's essentially inflammation, inflammatory diarrhea, together with 0:52 many other things, 0:54 such as ulcers, and really painful gut area. 0:59 Intomibah histolotica has two main forms. 1:05 One is assist form, which is the infective form. 1:09 It is spherical in shape with refractile walls. 1:12 Then we have the trophazoid form, which is the mobile form. 1:16 It is about 15 to 30 micrometers and is shaped like ameba, hence the name. 1:25 Let's look at how intomibah histolotica infects a human body by looking at its 1:32 life cycle 1:33 and how it causes amebic dysentery. 1:38 So, here I am drawing a human, and here is the GI tract. 1:42 I am drawing the gastrointestinal tract, the GI tract, because intomibah histol 1:48 otica enters 1:49 the body, predominantly through the mouth, and then goes through the digestive 1:53 tract, 1:54 causing its stuff. 1:57 Now, before continuing on, we must know that intomibah histolotica can cause 2:05 either an 2:06 invasive infection or a non-invasive infection. 2:12 A non-invasive infection occurs 90% of the time, and is obviously not as severe 2:20 as the name suggests. 2:21 However, an invasive infection occurs 10% of the time, which is a lot, and can 2:27 cause some serious problems. 2:32 So, we will first follow a non-invasive infection, which occurs 90% of the 2:41 cases, so intomibah histolotica 2:44 cysts are the effective form of this progzoa. 2:51 Ingestion of fecally contaminated water or food containing intomibah histolot 2:57 ica cysts 2:58 can be ingested through the mouth. 3:00 So these cysts can come from contaminated food or water, fecally contaminated 3:04 food or water. 3:06 The cysts will move through the mouth, down the esophagus, into the stomach. 3:12 Here, the cysts are in the stomach. 3:15 The cysts are resistant to the gastric environment, and just passes through 3:19 towards a small intestine. 3:22 So these cysts pass and move into the small intestine. 3:26 Each cyst can divide and produce 8 trophazoids, the mobile form of intomibah 3:32 histolotica, in the small intestine. 3:35 So this process is known as existation. 3:40 And this is where the cysts produce trophazoids in the small intestine. 3:46 These trophazoids will then move into the colon of the large intestines, where 3:51 it will establish colonization. 3:55 Let's zoom in and see what happens in a non-invasive infection by intomibah 4:02 histolotica. 4:04 Here is the colonic epithelial cells of the large intestines. 4:08 Here we have the mucus layer covering these epithelial cells. 4:13 The histolotica trophazoids will essentially just be on the surface of this muc 4:18 us and begin multiplying by binary fusion. 4:23 The trophazoids will colonize in the mucus layer and form new cysts. 4:29 This process is called endcystation, where it makes new cysts. 4:35 So here we have the trophazoids, which will just colonize the colon of the 4:39 large intestines and just produce a lot of cysts. 4:43 And this is the non-invasive infection. 4:46 The cysts will just exit out of the body in store, in the feces, and then the 4:51 cysts can infect new humans through contamination by contaminating food or 4:57 water. 4:59 So essentially, in the non-invasive infection, these trophazoids will live 5:04 within the human asymptomatically and might produce some discomfort and some 5:09 diarrhea. 5:10 But nothing invasive, hence the name, non-invasive infection, and the cysts 5:16 will just exit out of the body. 5:19 How about in an invasive infection? What happens then? Well, let's take a look. 5:27 So here, again, we have the colonic epithelial cells and the mucus. In an 5:39 invasive infection, the trophazoids will invade and colonize the colonic epit 5:41 helial cells. 5:42 And this will cause the epithelial cells to life, to die. And this will create 5:48 ulcers within the large intestines. 5:52 And of course, because they're trying to invade a cell within the body, there 5:56 will be an immune response. 5:58 For example, neutral fills will respond to the invasion and cause further 6:04 damage through lysing itself. 6:07 And so, essentially, this will aggravate the whole process and will create ul 6:11 cers, as you can see. 6:13 So the epithelial cells will start developing ulcers within the colon of the 6:17 large intestines. 6:19 And then it will just essentially damage this whole epithelial layer and mucus, 6:23 and then the trophazoid can then move into the bloodstream. 6:26 When in the bloodstream, the trophazoid can target other organs. 6:33 So, invasive infection is when the trophazoids through the bloodstream can 6:41 infect other organs, such as the liver, the lungs, and rarely the brain. 6:49 So, for example, this trophazoid can infect the liver, forming liver abscesses, 6:54 or it can form the lung, forming lung abscesses, which is not very common. 7:00 Or very rarely, it can go into the brain and form brain abscesses. It can cause 7:04 brain abscesses formation. 7:07 So, essentially, from all this, we know that the invasive infection, which 7:13 constitutes about 10% of anti-moema histolytica infections, is very serious. 7:20 It can cause definitely inflammatory diarrhea, which is a characteristic of amo 7:25 ebed dysentery. It can cause leukocytosis. 7:29 It can potentially cause amoebic liver abscess formation, and rarely lung and 7:34 brain abscesses. 7:36 It can also cause colitis and ulcers, which is exactly the same thing, ulcer 7:41 ative colitis, which is actually a very big characteristic of amoebic dysentery, 7:47 the ulcer formation in the large intestine, the colon. 7:51 And so, because of this, and because of inflammatory diarrhea, amoebic dysent 7:58 ery is characterized by blood and mucus in stool. 8:03 Now, how would you treat amoebic histolytica infections, especially the 8:07 invasive ones? 8:08 Well, you're treated with a group of drugs called azzles, particularly metronid 8:16 azole. 8:18 Diagnosis of anti-moema histolytica infection is through fecal examination of 8:24 cysts, because the cysts come out of the feces in stool. 8:29 So, from all this, we know that an intermoeba histolytica infection can be not 8:33 invasive or invasive, and can cause amoebic dysentery, which is pretty serious. 8:39 Thank you for watching this video. I hope you enjoyed it. Please like, share, 8:42 and subscribe. And comment.