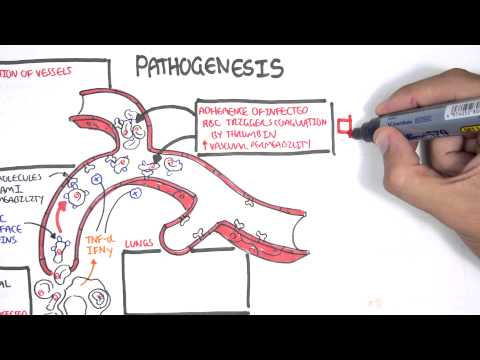
0:00 Meningitis is inflammation of the meninges, and the meninges are the layers 0:08 that surround 0:09 and protect our brain. 0:11 In this video, we're going to mainly focus on bacterial meningitis. 0:16 The main causative organisms of meningitis include group B streptococcus, stre 0:21 ptococcus 0:22 pneumoniae, nesseria meningitis, gram-negative bacilli, and hemophilus 0:28 influenza. 0:29 The reduction of the hemophilus influenza and pneumococcal vaccination have 0:34 decreased 0:34 infant-associated mortality due to meningitis. 0:38 The causative agents have to be in contact with the meninges in order to cause 0:43 meningitis, 0:44 but the meninges is essentially surrounded by the skull, because the meninges 0:49 itself 0:49 coats the brain. 0:51 Therefore, the infective organisms usually cause a primary infection first, or 0:57 they 0:58 can enter the area because of some abnormality or deformity of the skull. 1:04 So, for example, there can be a cribiform plate defect. 1:07 The primary infection can be otitis media, sinusitis. 1:11 There could be a basal skull fracture. 1:14 It could be secondary to pneumonia. 1:17 And all these primary problems can subsequently lead to meningitis. 1:23 So now let's look at the pathophysiology as to how the bacteria get from the 1:26 primary 1:26 problem here into the meninges and cause a problem. 1:31 Bacteria themselves poses virulent factors that help in four aspects in the 1:35 pathophysiology. 1:37 Colonization, invasion, immune evasion, and meningial invasion. 1:44 In order to learn about these four aspects of bacteria, virulence, let us 1:48 create a scenario. 1:49 In this scenario, we are going to look at the hematogenous spread of the 1:54 bacteria from 1:55 the primary source, or from the primary infection. 1:59 Here is the lumen of the nose, or gut, or the lungs. 2:02 And here is the mucus. 2:03 This is the epithelium. 2:05 And under the epithelium is the interstitial layer. 2:08 And then you have your capillaries, basically, your blood vessels, which then 2:12 circulates 2:13 all around your body. 2:15 The lumen is obviously an access point for the bacteria. 2:19 It can be in the ear, the gut, the nose, wherever. 2:25 Colonization refers to the bacteria's ability to colonize the area. 2:30 So for example, the bacteria strep pneumoniae and neccesiria meningitis have 2:35 the ability 2:35 to break down host antibodies using IgA proteases, which break down the mucosal 2:41 antibody IgA. 2:44 And these allow bacteria to colonize the area. 2:48 Some bacteria also have pilai, or fimbriae, allowing them to latch onto the 2:53 host's epithelium 2:54 and invade through. 2:56 We can say now that the bacteria has caused an infection, and we could say that 3:00 this is 3:00 the primary infection, be it pneumonia or sinusitis. 3:06 Some bacteria have virulent factors or mechanisms which allow them to evade the 3:11 immune system. 3:12 For example, the bacteria group B streptococcus and streptococcus pneumonia 3:18 have a capsule, 3:19 which allows it to evade macrophages as well as complement factors around the 3:24 area. 3:25 The bacteria can enter the bloodstream, causing bacteremia. 3:29 And then it can travel towards the brain. 3:31 And this is of course the hematogenous spread. 3:35 It's important to know that the bacteria can invade the meninges through hemat 3:39 ogenous 3:39 spread, so through the blood, directly. 3:42 So for example, from sinusitis, from abode infection, or it can go through the 3:48 cerebrospinal fluid 3:49 somehow. 3:50 And this is the scenario that we will look at. 3:53 Before continuing on with the pathophysiology, it's important to revise and 3:58 recap the anatomy 3:58 and physiology of the brain, specifically the cerebrospinal fluid. 4:04 The cerebrospinal fluid is the fluid produced by the brain, and it helps nour 4:08 ish the brain 4:09 tissues. 4:11 The cerebrospinal fluid, or CSF, is produced by the ventricles of the brain. 4:17 For simplicity, the fluid is produced by the lateral ventricles, which then 4:21 flows to the 4:22 third ventricles, then the fourth ventricles, and from the fourth ventricles, 4:27 it will enter 4:28 the subarachnoid space. 4:33 And from the subarachnoid space, it will go through the arachnoid granulation 4:39 and enter 4:40 the venous sinus. 4:42 And the venous sinus is essentially the big veins that will bring the blood 4:46 back down 4:47 to the heart. 4:50 The meninges that we've been talking about all this time are the layers above 4:55 and below 4:56 the subarachnoid space. 5:02 Now the arachnoid space itself also contains blood vessels, and there are even 5:07 blood vessels 5:08 which reach the ventricles of the brain. 5:11 And this is important because blood carries important things with it, and the 5:16 brain needs 5:17 these important things to function. 5:20 So let us compare blood vessels traveling to the ventricles, as opposed to 5:23 blood vessels 5:24 traveling around the brain. 5:28 The brain is actually ingeniously physically protected by the blood brain 5:33 barrier. 5:34 The blood brain barrier is a semi-permeable membrane barrier which really 5:39 separates circulation 5:41 and the brain tissue. 5:43 And it essentially prevents substances from getting inside the brain, because 5:47 as we know 5:48 the brain is such a delicate organ. 5:51 Blood vessels or the capillaries are of course made up of endothelial cells. 5:57 Surrounding the endothelial cells is the basement membrane, and surrounding the 6:01 basement membrane 6:03 are astrocytes, which are glial cells, which are the brain's supporting cells. 6:11 And this formation allows only certain things to pass through inside the brain. 6:17 So the blood brain barrier allows glucose and oxygen to get inside the brain, 6:21 because 6:22 the brain obviously needs glucose for energy and oxygen as well. 6:28 If we compare the blood brain barrier to the blood cerebrospinal fluid barrier, 6:32 where 6:33 the ventricles are, the capillaries are made up of endothelium as well, and are 6:38 surrounded 6:39 by the basement membrane. 6:41 But here there are no astrocytes. 6:43 Rather, there are these other supporting cells called epidymal cells, which are 6:47 the cells 6:48 responsible for the production of cerebrospinal fluid inside the ventricle 6:55 cavity. 6:56 So cerebrospinal fluid is produced by the choroid plexus, which is essentially 7:00 epidymal 7:01 cells, and circulate around the brain as we have learned. 7:06 Because the choroid plexus is the site of cerebrospinal fluid production, more 7:11 blood products 7:12 are able to move here. 7:15 So for example, glucose can enter, oxygen, ions, and even vitamins can get into 7:19 this 7:19 area. 7:21 Sadly though, bacteria can also get here. 7:25 And there can invade the meninges through this mechanism. 7:30 What is very interesting here is that cerebrospinal fluid is so sterile. 7:35 There is inadequate humoral immunity. 7:37 There is low immunoglobulins here, and there's low complement proteins. 7:41 And so you can imagine the hematogenous spread, the bacteria can enter the vent 7:46 ricles and 7:46 then enter the cerebrospinal fluid. 7:52 Now it is important to again recap the cerebrospinal fluid flow around the 7:57 brain and look at it 7:59 in a bit more detail. 8:00 So let's say the bacteria are in the lateral ventricles. 8:04 They can move to the third ventricles via the interventricular foramen, then 8:08 into the 8:09 fourth ventricles via the cerebral aqueduct, then again gain access to the sub 8:14 arachnoid 8:15 space through the medial and lateral apertures. 8:19 And this is where the bacteria really want to be, I guess, because they are now 8:23 surrounded 8:23 by the meninges, and so it can trigger meningitis through an inflammatory 8:29 reaction. 8:30 To make this story complete however, the cerebrospinal fluid can continue and 8:35 be reabsorbed into 8:36 the venous sinus via the arachnoid granulation, and from the venous sinus back 8:41 into circulation, 8:43 back to the heart. 8:45 On a side note, the fourth ventricle also continues on down the spinal cord 8:49 because the 8:50 cerebrospinal fluid also needs to supply the spinal cord with its goods, but 8:55 the focus 8:55 of our story is the subarachnoid space. 9:00 So let's just orientate ourselves as to where the subarachnoid space is. 9:06 So here is the skull, your skull bone, the outside, I guess, below your skull 9:10 is the 9:10 duromata, below that is the arachnoid membrane, and then the arachnoid space, 9:17 which is a 9:18 lot of spider-webby-like projections, remember, we said that the arachnoid 9:23 space also contains 9:24 blood vessels. 9:25 The blood vessels travel also deep between the brain sulkyte to supply it with 9:29 oxygen 9:30 and glucose. 9:32 Below the arachnoid space is the piamata, and finally below the piamata is the 9:37 brain 9:37 parenchima, the brain tissue, the clean slate, the tabula rasa. 9:44 The piamata, arachnoid membrane and the duromata make up the three layers of 9:48 the meninges. 9:50 The meninges are pain sensitive, particularly the duromata. 9:56 Let us now zoom and focus on this area again, the subarachnoid space. 10:04 In this diagram on the left side you have the vasculature, the circulation in 10:09 the arachnoid 10:10 space. 10:11 And then on the right you have where the cerebrospinal fluid is traveling and 10:16 where bacteria are 10:16 right now. 10:20 Bacteria in the cerebrospinal fluid can use up the glucose in the area and use 10:24 glucose 10:24 as a source of energy. 10:26 So in the cerebrospinal fluid now we have the bacteria. 10:32 Now the vasculature will respond to the presence of bacteria and will increase 10:39 the vessel wall 10:41 permeability. 10:42 You have also a decrease in perfusion pressure and possibly subsequent ischemia 10:48 . 10:48 There will be increase in adhesion proteins for leukocytes to allow it to 10:53 invade the area 10:55 and also you will actually have endothelial damage, so vessel damage in 10:59 response to cytokine 11:01 mediated inflammation. 11:03 So let's talk about each of those points. 11:05 So for example you have neutrophils entering the area thanks to an increase in 11:10 vascular 11:10 permeability and adhesion proteins. 11:13 They essentially cause inflammation, they trigger inflammation, they release so 11:18 many 11:18 cytokines. 11:20 Macrophages also enter the area and cause inflammation. 11:24 It's important to note that macrophages also use glucose as a source of energy. 11:31 Because there is an increase in vascular permeability, water and proteins can 11:35 leak inside the subarachnoid 11:37 space causing cerebral edema and subsequently increasing intracranial pressure. 11:44 Therefore, if you were to perform a lumbar puncture on someone you suspect to 11:49 have a bacterial 11:50 meningitis, in the cerebrospinal fluid from the lumbar puncture you would find 11:56 bacteria 11:57 increase in proteins, increase in neutrophils and decrease in glucose. 12:03 Due to the irritation and inflammation of the meninges, the classical signs and 12:06 symptoms 12:06 of meningitis include fever, headache, photophobia, nausea, vomiting, next 12:13 stiffness. 12:14 We of course looked at the hematogenous spread of bacteria into the subarachn 12:20 oid causing 12:21 meningitis. 12:22 However, the bacteria can also locally invade the meningitis, for example 12:27 through the sinuses. 12:29 As well, it can invade into brain tissue through normal circulation straight 12:34 into the subarachnoid 12:36 space via the vessels within the subarachnoid space.