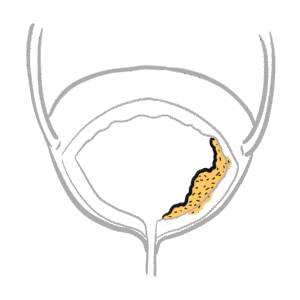
0:00 Hello, in this video we are going to talk about bladder carcinoma. 0:07 This is an overview and introduction. 0:10 Bladder carcinoma is a common urogenital cancer. 0:14 It is common in the elderly and is strongly associated with smoking. 0:21 Here I am drawing a middle-aged person in the toilet urinating. 0:28 We are going into the presentation of bladder cancer. 0:32 It's important to revise the anatomy. 0:35 Here is the kidney, the ureter, which brings urine into the bladder where urine 0:41 is stored. 0:43 When the bladder is full, urine passes through the urethra and goes out. 0:51 There is the prostate below the bladder in men and in women, there is the 0:58 uterus which 0:59 is behind the urinary bladder. 1:04 Here is a growth in the bladder which signifies or represents carcinoma. 1:11 Let us compare the normal bladder and look at its progression to carcinoma of 1:17 the bladder. 1:18 The most common carcinoma is urotheleoma, which is tumor from the urotheleum. 1:28 This type of cancer is sometimes referred to as transitional cell carcinoma 1:32 because at 1:33 the end of the day these are transitional cells. 1:37 So let us look at the layers of a normal bladder. 1:41 This is the lumen of the bladder where urine is stored. 1:46 The inner layer of the bladder is called the urotheleum and it is made up of 1:51 transitional 1:52 epithelial cells. 1:55 Below it is the basement membrane, which separates the transitional cell epit 2:01 helia with the laminopropia. 2:04 The laminopropia consists of many blood vessels. 2:08 Below the laminopropia is the detruser muscle and then we have the adventicia, 2:13 which is 2:13 primarily fat. 2:19 The cells within the urotheleo layer which are made up of transitional cells 2:24 can evolve 2:25 and mutate due to several factors and this will lead to abnormal cells and then 2:34 progress 2:35 to urotheleoma or transitional cell cancer. 2:41 There are a few types of urotheleomas, there is carcinoma in situ, which is 2:47 essentially 2:48 carcinoma confined to that layer. 2:53 You have a cesal tuma or a pillory tumas which project out. 3:02 These tumas can then subsequently keep growing and actually grow deeper and 3:06 penetrate the 3:07 other layers under it. 3:10 This is where it becomes dangerous. 3:15 The risk factors for developing bladder cancer, especially urotheleoma, is 3:20 smoking. 3:21 Exposure to certain chemicals, which won't be discussed, cyclophosphamide, a 3:27 medication, 3:28 aristolucic acid, age greater than 40, and there are some other minor risk 3:36 factors, which 3:38 are not mentioned. 3:40 The signs and symptoms of bladder cancer include hematuria, mainly, with or 3:47 without pain. 3:50 It's usually painless hematuria and presentation of this should always ring 3:55 alarm bells, especially 3:57 if in the presence of the other risk factors, such as age. 4:02 Other signs and symptoms can include renal colic, there can be blood clots in 4:08 the urine. 4:09 Resuria, frequency, urgency, and urinary retention. 4:17 There can be systemic signs of malignancy, including fever, weight loss, and 4:26 night sweats. 4:27 And therefore, the investigation to order upon such presentation is you can do 4:33 a bedside 4:34 urine analysis, urine cytology to actually look at malignant cells, full blood 4:41 count 4:41 to check for anemia, EUCs to check for electrolyte urea creatinine, which is a 4:48 good marker for 4:49 kidney function, CRP, which can identify signs of malignancy, inflammation, or 4:55 infection. 4:57 The ultrasound of the bladder and kidney is a very good investigation for 5:01 imaging. 5:02 Finally, there is invasive cystoscopy, which is gold standard, actually. 5:07 And this is where the bladder can be visualized from within, so you can see the 5:13 urotheleolayer. 5:14 And also with this, a biopsy can be formed of the growth, of the tumor, and 5:19 this can 5:19 be subsequently examined. 5:24 The most common types of bladder cancer is urothele carcinoma, as I mentioned, 5:29 which 5:30 is the most common. 5:31 And this is also known as transitional cell carcinoma. 5:35 There are also other types of bladder cancers, including squamous cell carcin 5:43 oma and adenocosinoma. 5:46 After obtaining the biopsy of the tumor within the bladder, the tissue is 5:51 examined for malignancy, 5:53 whether it's present or not. 5:56 If malignancy is confirmed, the next step is to stage the tumor, because this 6:01 will then 6:02 tailor the management. 6:04 The use of PET scan, or CT scan, can help stage the bladder tumor accurately, 6:10 and to 6:10 see what layers of the bladder are involved, and to see if the tumor has spread 6:15 elsewhere 6:16 around the body. 6:18 So let us recap the layers of the urinary bladder. 6:24 Here on the top is the bladder lumen, again which stores urine. 6:31 The urotheleum, which is composed of the transitional epithelial cells, below 6:37 this is the basement 6:38 membrane. 6:40 The laminopropia under it, and then you have the muscle layer called the detre 6:45 user muscle, 6:46 and there's an inner and outer part for a superficial and deep. 6:51 The lower the detreuser muscle is the adventicia, which is the fat layer. 6:58 The World Health Organization staging of bladder tumours include low malignancy 7:04 potential, 7:05 which include carcinoma and situ, or TA, which include cecile or papillary tum 7:14 ours. 7:15 The low malignancy potential make up the majority of bladder tumour. 7:22 After low malignancy potential, the World Health Organization has the low grade 7:29 stage, 7:30 which is where the bladder tumour has grown to the deeper layers. 7:36 And this is T1. 7:38 T1 involves the growth, reaching the basement membrane and the laminopropia. 7:44 There's T2A, where the tumour goes past the laminopropia, and invades the 7:50 superficial 7:51 muscle layer. 7:54 The high grade stage includes T2B, which is where the tumour has extended all 8:02 the way 8:03 towards the deep layer of the detreuser muscle. 8:07 T3 is where the tumour has invaded the perivesicle tissues. 8:13 T4 is tumour invading adjacent organs, or the tissues of those organs. 8:20 From here, the tumour can metastasise via hematogenous spread, local spread or 8:29 lymphatic 8:30 spread. 8:35 The staging of the bladder tumour into low grade and high grade is important. 8:43 It is important because this will tailor the treatment. 8:50 And the treatment will depend on if the tumour has invaded the muscle layer or 8:56 not. 8:57 So the management, the treatment, focuses on non-muscle invasive disease and 9:04 muscle invasive 9:05 disease. 9:08 Muscle invasive disease has poorer prognosis. 9:15 In non-muscle invasive disease, treatment options include TURBT or Terb-T, 9:21 where you 9:22 resect the tumour essentially. 9:26 Or there is a method called intravusicular chemotherapy, where the chemotherapy 9:32 agent 9:33 in liquid form is injected into the bladder and acts locally there. 9:39 Finally, there is cystectomy, which is removal of the bladder. 9:46 This of course means that the ureter, which brings urine down to the bladder, 9:51 has to be 9:51 reconnected somewhere so that urine can go out somewhere else. 9:56 Now let's focus on muscle invasive bladder carcinoma, which as mentioned has a 10:01 poorer 10:02 prognosis. 10:04 Here the patient undergoes neo-adjuvant chemotherapy prior to surgery. 10:09 Surgery will involve radical cystectomy, which is removing the bladder. 10:15 This will be followed by urinary diversion. 10:20 This urinary diversion is done in order to divert the urine flow elsewhere. 10:28 And this can be done by taking part of the small intestine, joining it with the 10:32 ureter 10:33 and creating a stoma, or the ureter can drain into the lodging test time. 10:41 Post-surgery chemotherapy is used again. 10:46 The chemotherapy of choice nowadays is this platen and five flora uracil. 10:52 However radiation is also offered with chemo for bladder cancer, and thus chemo 10:58 agents 10:58 used vary.