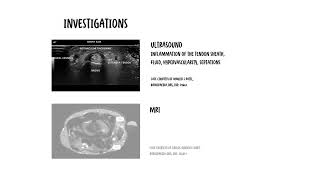
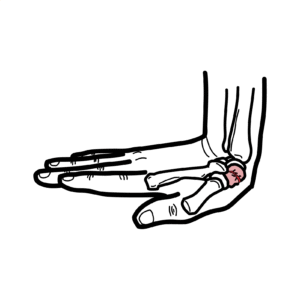
0:00 Decrovein's Tino-Sanovitis is a common painful condition affecting the tendons 0:18 on the thumb 0:18 side of the wrist. 0:20 It occurs when the tendons that help move the thumb, specifically the Abductor- 0:25 Policis 0:26 longest APL, and extensor Polysis Brevis EPB, become irritated and thickened as 0:34 they pass 0:35 through a narrow tunnel, the first dorsal compartment at the wrist. 0:41 This irritation leads to swelling, restricted tendon gliding and pain, 0:45 particularly with 0:47 thumb movement or gripping. 0:49 It is frequently seen in people who perform repetitive thumb or wrist motions 0:54 and is also 0:55 common in new parents and caregivers due to repeated lifting and holding. 1:06 Anatomically, the condition involves the first dorsal compartment of the wrist, 1:09 as mentioned. 1:10 A narrow, fibrous tunnel located on the radial, the thumb side of the distal 1:17 forearm. 1:18 This compartment contains two key tendons, the Abductor-Policis Longus APL, 1:23 which abgucts 1:25 and assists with extension of the thumb, and the extensor-Policis Brevis EPB, 1:32 which extends 1:33 the thumb at the metacarpal phalangeal joint. 1:37 These tendons are normally surrounded by a synovial sheath that allows smooth 1:40 gliding 1:41 during thumb and wrist movement. 1:43 Anatomical variations are common, many individuals have multiple Abductor-Polic 1:48 is Longus tendon 1:49 slips or a septum separating the Abductor-Policis Longus and extensor-Policis 1:55 Brevis, which can 1:56 predispose to tendon crowding and impaired movement within the compartment. 2:03 Decovane's Tino-Sanovitis, which is Tino-Tendon-Sanovitis Inflammation of the 2:10 synovial sheath, which surrounds 2:11 the tendon, is associated with repetitive manual tasks, smartphone you overuse 2:18 for example, 2:19 and caregiving activities, particularly those involving sustained thumb 2:24 abduction and wrist 2:25 deviation. 2:28 Education on ergonomics pacing and early symptom recognition is important to 2:32 prevent chronicity. 2:39 From a pathophysiological perspective, Decovane's Tino-Sanovitis is now 2:43 understood to be more 2:45 of a degenerative or stenosing tendonopathy, rather than a purely inflammatory 2:51 condition. 2:52 Histological studies have shown mixoid degeneration and thickening of the 2:56 tendon sheath rather 2:57 than classic inflammatory cell infiltrates, where you would see autoimmune 3:07 conditions. 3:09 Clinically patients typically present with pain and tenonus over the radial 3:15 thumb side 3:15 of the wrist, which may radiate into the thumb or forearm. 3:22 Pain is often exacerbated by thumb movements, pinching, gripping, lifting 3:26 objects or twisting 3:28 motions such as opening jars. 3:32 Swelling over the affected area may be visible, and some patients report cre 3:37 aking or catching 3:39 sensations with thumb movement. 3:42 A hallmark clinical test is the Finkelstein test, where the thumb is flexed 3:50 into the palm 3:53 and the wrist is deviated towards the ulna. 3:57 Reproduction of sharp pain over the radial wrist is highly suggestive of the 4:06 diagnosis. 4:08 Then we have investigations, here in the first image we're looking at an 4:13 ultrasound of the 4:14 wrist, in a short axis view over the radial side. 4:19 First here is the dorsal compartment, the first compartment. 4:26 Inside this, compartments sit two tendons, the abductor polysis longest and the 4:30 extensor 4:31 polysis brevis. 4:33 In Decovane's, what we're looking for is inflammation of the tendon sheath. 4:37 There are few key ultrasound findings beginners should recognize. 4:42 Thickening of the retinaculum, the roof over the tendons become swollen, this 4:47 you can see 4:48 on this particular image. 4:50 Fluid around the tendons you'll often see as a dark rim, hyper-fascularity on 4:55 Doppler, 4:55 meaning you get increased blood flow. 4:59 Sometimes you can see septations where the compartment is split into subcomp 5:03 artments. 5:04 All of these features point towards Tino-sanovitis of the first dorsal 5:08 compartment which is Decovane's. 5:12 Now let's move on to MRI, here is an MRI slice through the wrist. 5:17 Here we can see the tendons of the first dorsal compartment or the first ext 5:22 ensor compartment 5:23 labeled APL and EPB. 5:28 Abductor polysis longest and extensor polysis brevis. 5:31 In MRI we're looking for fluid around the tendons, thick in tendon sheath and 5:36 soft tissue swelling. 5:38 But MRI isn't usually needed to diagnose Decovane's, instead we use MRI when we 5:43 want 5:43 to exclude alternative diagnosis or look for deeper pathology or if symptoms 5:48 are not really 5:48 responding to basic treatment. 5:56 Intersection differentials include thumb, carpal, mericarpal osteoarthritis, 6:01 intersection syndrome. 6:04 Intersection syndrome is essentially an inflammatory problem that occurs at the 6:10 tendons at the 6:11 back of the forearm relatively close to where you find Decovane's. 6:18 Another differential include radial-sensoring nerve entrapment, also known as W 6:22 artenberg syndrome, 6:24 and Schaeford pathology. 6:31 Management of Decovane's is typically step-wise and depends on symptoms 6:34 severity and duration. 6:36 First line treatment is activity modification to reduce aggravating movements, 6:41 use of thumb 6:42 speaker splint to limit thumb and wrist motion, a short-term analgesia such as 6:48 paracetamol 6:49 or non-steroidal anti-inflammatory drugs if appropriate. 6:53 Corticosteroid injection into the first dorsal compartment is highly effective, 6:59 with symptoms 7:00 resolve in majority of patients after one or two injections, particularly when 7:05 accurately 7:05 placed. 7:07 Ultrasound guidance may improve outcomes in anatomically complex cases. 7:11 Physiotherapy focusing on load modification, gentle tendon gliding and erg 7:15 onomic advice 7:16 can be useful at junk. 7:19 For patients with persistent or recurrent symptoms, despite these conservative 7:23 management, surgical 7:25 reefs of the first dorsal compartment may be considered, and this involves 7:29 decompression 7:30 of the tendon sheath and division of any septations allowing free tendon 7:36 movement. 7:38 Overall, the prognosis is good, especially with early diagnosis and appropriate 7:46 treatment, 7:47 and most individuals can expect a full return to function. 7:57 So in summary, decovanes is really a common problem, particularly in new 8:02 parents, caused 8:04 by repetitive lifting and holding, which causes essentially irritation of two 8:10 tendons, abductor 8:11 polysis long-bus and extensor polysis brevis.