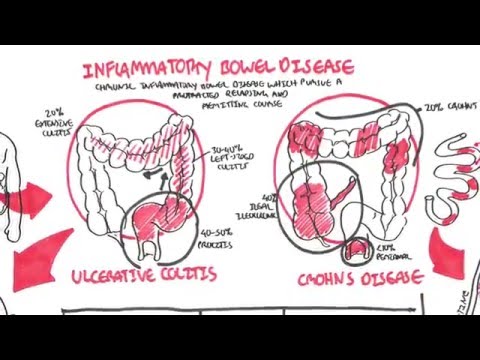
0:00 Gourd, also known as gastroesophageal reflux disease, is one of the most 0:11 prevalent gastrointestinal 0:13 disorders. 0:14 Some stats show that up to 15% of individuals have heartburned and/or regurg 0:18 itation at least 0:19 once a week. 0:21 Symptoms are caused by backflow of gastric acid and other gastric contents into 0:25 the esophagus, 0:27 due to incompetent barriers at the gastroesophageal junction. 0:31 As you can see, as demonstrated by this diagram, content from the stomach is 0:35 going back up 0:36 and irritating the esophagus. 0:39 Let's recap some anatomy. 0:41 Eosophagus can be divided into the upper 2/3 and lower 3rd. 0:46 It's divided like so because there are some noticeable differences between them 0:50 . 0:50 The upper 2/3 of the esophagus contains stratified skeletal muscles, whereas 0:56 the lower 3rd contains 0:57 all smooth muscle, and so it is not under voluntary control. 1:03 The mucosal surface of the upper 2/3 is non-caratinized stratified squamous 1:08 epithelial cells, whereas 1:10 the lower 3rd there is transitional or stratified squamous epithelium to simple 1:17 columnar epithelium. 1:19 This squamous columnar junction has a zigzag appearance, thus sometimes 1:25 referred to as 1:25 the Z line. 1:27 The Z line again is a change from the squamous epithelium to the columnar epit 1:32 helium. 1:33 Fortunately, there is an esophageal sphincta, which is a barrier for food and 1:37 acid from 1:38 going backwards from the stomach up to the esophagus. 1:42 However, when the sphincta is incompetent, good results. 1:48 It's important to recap some basic physiology of acid production in the stomach 1:53 here. 1:54 The stomach is made up of pits, which houses many different cells. 1:59 Imagine here is your stomach lumen. 2:02 These cells of the stomach include mucous cells, parietal cells, enterochrom 2:07 ophen cells, and 2:08 some other hormone cells which I have not drawn. 2:12 Parietal cells are the important cells which produce hydrochloric acid. 2:16 Now, there are two important channels for these cells. 2:22 One is the proton pump, which is an anti-porter, pumping hydrogen ions out in 2:29 exchange for 2:30 potassium ion. 2:32 The other channel is a simporter, which pumps both potassium and chloride. 2:39 Thus, with hydrogen and chloride in the lumen, this forms hydrogen chloride, 2:45 which helps 2:46 in digestion of food. 2:48 Many things can stimulate parietal cell activity and thus stimulate acid 2:53 production. 2:54 These include enterochromophen cells which release histamine. 2:58 Histamine binds onto histamine receptors on parietal cells, stimulating hydro 3:02 chloric release. 3:06 So that was some basic gastric physiology. 3:09 And the lower gastroesophageal sphincter is compromised due to a variety of 3:14 factors, 3:15 gourd results, or reflux disease results. 3:18 These factors include things that increase intra-gastric volume pressure. 3:25 And these things include chronic coughing, large meals, and delays in gastric 3:34 emptying. 3:35 Other factors include things that decrease the esophageal sphincter tone, which 3:40 includes 3:40 alcohol, search and medications or drugs such as tricyclic antidepressants, pep 3:47 tic strictures, 3:48 previous surgeries, and idiopathic causes. 3:53 Scleroderma is also another important cause of lower esophageal sphincter 3:59 incompetency. 4:00 Proderma is a condition characterized by thickening of tissue. 4:09 Now let's talk about the pathological features of gourd. 4:13 Gourd is further complicated by reflux esophageitis, which develops when the 4:18 mucosal defenses 4:19 are unable to counteract the damage done by acid, pepsin, and bile. 4:25 This causes inflammation of the esophagus. 4:28 The other important pathological change that can occur is also a complication. 4:33 These are esophageal strictures or peptic strictures. 4:36 Asophageal strictures results from fibrosis that causes luminal constriction. 4:42 These strictures occur in 10% of patients with untreated gourd, and also 4:47 present in 4:48 the distal esophagus near the squamocolumina junction. 4:52 The clinical presentation or the classic presentation signs and symptoms of g 4:57 ourd, reflux disease, 4:58 is a classic heartburn and angina type pain, worse after meal and worse lying 5:05 down. 5:05 It's also characterized by acid brash or water brash, and also sometimes organ 5:11 ophagea, which 5:12 is pain when swallowing. 5:15 Reflux into the pharynx larynx and tracheobronkyl tree can cause chronic cough, 5:21 laryngitis, 5:22 sinusitis, morning hoarseness may also be noted. 5:27 Many patients with gourd remain asymptomatic and do not seek attention until 5:32 severe complications 5:33 usually occur. 5:35 The diagnosis of reflux disease is easily made by history alone. 5:40 Diagnostic studies are indicated in patients with persistent symptoms or 5:44 complications, 5:45 or those who do not respond to therapy. 5:48 If patients are under the age of 45, gourd is suspected, and a trial of proton 5:53 pump inhibitors 5:54 are given. 5:56 If they fail with treatment, investigations are warranted. 6:00 For people greater than 45 years old and have reflux, trial of PPI, which are 6:06 proton 6:06 pump inhibitors, can be given, or other investigations can be done, especially 6:11 if you are suspicious 6:13 of complications associated with gourd. 6:16 A gastroscopy, where an endoscope camera is inserted down the esophagus for 6:20 visualizing 6:21 any changes, can also be performed. 6:24 Although endoscopy is sensitive for diagnosis of esophageitis, it can miss 6:28 causes of reflux, 6:30 since some patients have symptomatic reflux without esophageitis. 6:34 A less invasive investigation is barium swallowing study, where patients drink 6:40 contrast and ask 6:41 to swallow. 6:42 This process is captured by x-ray. 6:45 Usually it is normal, and abnormal when complications such as bad esophageitis 6:49 and strictures are 6:50 present. 6:51 A 24-hour ambulatory pH monitor can be used, which is the most sensitive test 6:58 for diagnosing 6:59 gourd. 7:01 Again, the most sensitive test for diagnosis of gourd is the 24-hour ambulatory 7:07 pH monitoring. 7:09 The goal of treatment of gourd is to provide symptom relief, heal erosive esoph 7:14 ageitis, 7:15 and prevent complications. 7:17 Management of mild cases of gourd include lifestyle changes, these include 7:22 weight loss, 7:23 smoking sensation, eating small regular meals, avoiding meals before sleep, 7:28 avoiding search 7:29 and food and drinks, such as fizzy drinks, avoiding alcohol, coffee, citrus 7:35 fruits and 7:36 spicy foods. 7:38 Pharmacological management is first-slide for suspected gourd, and is used in 7:44 conjunction 7:44 with lifestyle modification. 7:49 Pharmacological management aim to reduce acid production. 7:53 These include proton pump inhibitors, which inhibit the proton pump we talked 7:57 about, and 7:58 thus inhibit the release of hydrogen ions. 8:02 The other medication include antacids, which aim to neutralize hydrochloric 8:08 acid. 8:08 Another drug not commonly used are histamine receptor antagonist, which inhibit 8:14 the histamine 8:14 receptors, and thus inhibit the stimulation of parietal cells by the enteroch 8:19 romophen 8:20 cells. 8:21 Finally, there is a surgical management, and this is usually left when medical 8:25 management 8:26 has failed, and should be considered as an alternative for patients who require 8:30 long-term 8:31 high-dose proton pump inhibitors. 8:34 The anti-reflux surgery is known also as the Nissen's operation. 8:41 In this operation, the gastric fundus is wrapped around the esophagus, fundopl 8:47 ication, and 8:48 this increases the lower esophageal schfinkter pressure. 8:54 Finally, let's talk about the complications of gourd, and usually a 9:01 complication of esophageitis. 9:04 So these include complications, esophageitis, which is inflammatory changes in 9:08 the squamous 9:09 line esophagus. 9:11 This inflammation can cause dysphagia, and can cause metaplasia, a condition 9:18 termed barots 9:19 esophagus. 9:24 Barots esophagus is characterized by changes of squamous cells to columnar 9:29 cells, as well 9:30 as increased number of goblet cells in the area. 9:34 Barots esophagus is important because people with barots esophagus are at a 30- 9:40 125 time 9:41 risk of developing esophageal adenocarcinoma than the general population. 9:47 Other complications include stricture formation, ulcers, erosive esophageitis, 9:53 and of course 9:54 if bleeding occurs, iron deficiency can occur.