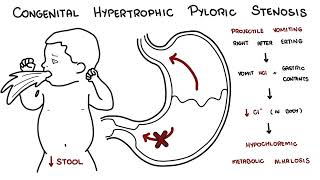
0:00 Congenital hypertrophic palaric stenosis is a problem found in babies. 0:11 It's where you get mocked thickening of the smooth muscle, or hypertrophy, in 0:15 the pylorus 0:16 that affects more male infants than female infants. 0:20 In babies with pylaric stenosis, the elongated, overgrown pylorus is hard, and 0:26 the pyloric 0:27 canal is narrow, resisting gastric emptying. 0:31 Approximately, the stomach may become dilated, hypertrophic palaric stenosis 0:36 presents with 0:37 projectile vomiting right after eating. 0:45 Let us review the anatomy of the stomach and the pylorus first. 0:49 The stomach has a shape of an expanded J, consisting of a short lesser curv 0:54 ature forming 0:55 the medial surface of the organ, and the long, greater curvature forming the 0:59 lateral surface. 1:01 The function of the stomach is to receive bolus, or the food, from the esoph 1:05 agus, then chemically 1:06 and mechanically prepares it for further digestion and absorption in the 1:11 intestine. 1:11 The stomach produces gastric juices, which gradually converts a massive food 1:17 into a semi-liquid 1:17 mixture, chime. 1:20 The chime then passes fairly quickly into the duodenum, the first part of the 1:25 small intestine. 1:26 We can divide the stomach into four regions, the cardia, fundus, body, and pyl 1:32 orus. 1:33 The pylorus is important. 1:35 The pyloric anterum, the wider part, leads to the pyloric canal, its narrower 1:42 part. 1:42 The pylorus contains large, circular, smooth muscles, which forms the pyloric 1:49 sphincter 1:50 and the pyloric orifice. 1:54 Intermittent emptying of the stomach occurs when the intra gastric pressure 2:00 overcomes 2:01 the resistance of the pylorus, and so at irregular intervals when the gastric 2:06 peristalsis, when 2:07 it contracts, it pushes the food, the chime, through the pyloric canal and or 2:13 ifice into 2:14 the small intestine, for further mixing, digestion, and absorption. 2:20 So that was a general anatomy, and some of the physiology of the stomach, as 2:24 well as 2:25 the pylorus. 2:28 As mentioned, congenital hypertrophic pyloric stenosis is a marked thickening 2:33 of the smooth 2:33 muscle in the pylorus. 2:37 The incidence is 3 in 1000 live births, and increases with familial risk. 2:44 Normally, gastric peristalsis, the contraction, pushes chime through the pyl 2:49 oric canal, and 2:50 orifice into the small intestine at irregular intervals. 2:55 In babies with pyloric stenosis, the overgrown elongated pylorus is hard, and 3:01 the pyloric 3:02 canal is narrow, resisting gastric emptying. 3:05 Approximately the stomach may become dilated. 3:11 Hypertrophic pyloric stenosis presents with projectile vomiting right after 3:15 eating, and 3:15 when you vomit, you vomit hydrochloric acid in the gastric contents. 3:21 Due to the loss of the hydrochloric acid in the gastric contents from 3:27 persistent vomiting, 3:29 these are at risk of electro imbalance, specifically characteristic hypochlor 3:37 amic metabolic alkalosis. 3:39 Babies tend to appear active and hungry, especially after vomiting. 3:44 There is also reduced stool, pool weight gain. 3:48 There's also something called a test feed. 3:50 A test feed is usually performed, so you can palpate a pyloric mass or tuma. 4:00 So diagnosis and investigation. 4:03 If pyloric, tuma, or mass is felt, no radiological investigations is necessary 4:08 prior to surgery. 4:10 Ultrasounds may show thickening, greater than 4 mm, elongated greater than 16 4:16 mm, pyloric 4:17 muscle, and increased muscle to lumen ratio, with decreased movement of fluid 4:22 through the 4:23 narrow canal. 4:26 Blood tests will reveal low sodium, low potassium, and low chloride and 4:31 elevated pH. 4:32 You get hypochloramic metabolic alkalosis from all the vomiting the baby is 4:41 doing. 4:43 In terms of treatment, well, correction of the hypochloramic alkalosis and hyp 4:47 ochlamia 4:48 is important, and nasogastric tube can be performed to drain content, to 4:55 prevent aspiration 4:56 of vomited secretions. 4:59 Fundamentally surgical treatment is gold standard. 5:01 This is termed pyloromyotomy, where you essentially cut up the pyloric muscle 5:07 fibers, allowing 5:08 the actual orifice to be larger. 5:18 So in summary, congenital hypertrophic pyloric stenosis is a problem in babies 5:23 characterized 5:23 by projectile vomiting after eating. 5:26 It's where you get thickening or hardening of the smooth muscle, hypertrophy of 5:30 the pylorus. 5:33 Management is surgery. 5:35 Thank you for watching. 5:48 [BLANK_AUDIO]