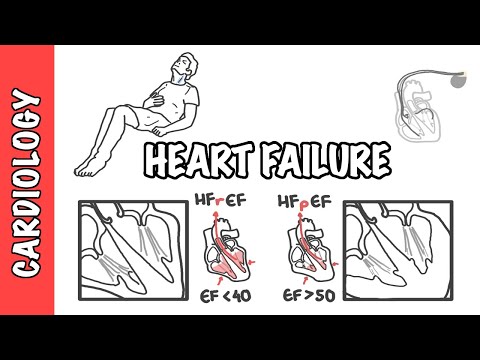
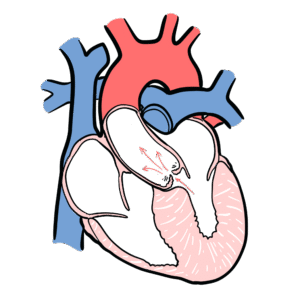
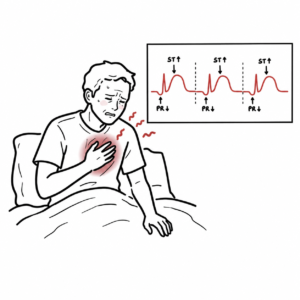
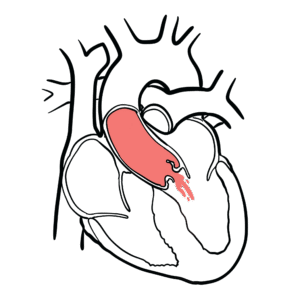
0:00 Takatsubo cardiomyopathy, also known as stress cardiomyopathy or apical balloon 0:15 ing syndrome, 0:18 is a hard condition often preceded by a stressful event such as a death of 0:22 someone or a recent 0:23 traumatic event. 0:29 The term Takatsubo is taken from the Japanese name for an octopus trap, which 0:36 has a shape 0:37 that is similar to the systolic apical ballooning appearance of the left vent 0:43 ricle. 0:44 Takatsubo cardiomyopathy is a clinical syndrome associated with reduced eject 0:49 ion fraction 0:50 of the heart, elevated cardiac enzyme levels, and signs of ischemia on ECG, but 0:58 in the actual 0:59 absence of angiographic evidence of obstructive coronary artery disease or 1:06 acute plaque rupture. 1:09 The pathophysiology of Takatsubo is unknown. 1:12 Takatsubo typically occurs in older women and is usually precipitated or 1:17 triggered by a 1:18 stressful physical event such as a full motor vehicle accident, as well as an 1:26 emotional 1:28 stressful event such as a death of someone, financial hardships, relationship 1:34 breakdowns. 1:35 The postulated mechanisms of Takatsubo include catacolamine excess following 1:41 one of these 1:42 stressful events, recent stresses stimulate sympathetic activity, resulting in 1:50 release 1:50 of catacolamines leading to increased vasoconstriction, heart rate, and 1:56 contractility of the heart. 2:01 These changes results in microvascular dysfunction as well as microvascular sp 2:07 asms, and this 2:08 is thought to result in myocardial stunning. 2:12 There can also be direct catacolamine associated myocardial toxicity, and all 2:18 of these things 2:19 will essentially manifest as symptoms of heart attack. 2:25 The other theory is an underlying microvascular dysfunction with coronary 2:31 artery spasm, again 2:33 manifesting as heart attack. 2:39 The typical patient with Takatsubo cardiomyopathy is a post-menopausal woman. 2:46 Women are much more affected than men, and the risk also increases with age. 2:53 So these people often present with acute or sub-acute onset of chest pain and 2:56 shortness 2:57 of breath, often with dizziness and occasional syncope, and this is all usually 3:03 in the context 3:04 of a recent stressor. 3:11 On ECG there are non-specific ST changes, elevation or depression with T-wave 3:22 changes. 3:23 Blood tests also show elevated troponins. 3:30 Because of these acute events, they often resemble an acute coronary syndrome, 3:34 a heart 3:35 attack, and so treatment would always be treatment for acute coronary syndrome, 3:41 and an emergent 3:42 coronary angiogram is often performed. 3:47 And in Takatsubo's cardiomyopathy will demonstrate non-obstructive coronary 3:52 artery disease. 3:55 On angiogram, you can also visualize that during diastole the ventricles are 4:02 filling 4:02 with blood, but during systole the apical section of the ventricular cardiomy 4:09 ocyte is hypokinetic. 4:11 It's not really working. 4:13 And this is the most common form of Takatsubo cardiomyopathy. 4:21 So by using an echocardiogram, you can also see features of Takatsubo. 4:26 There is systolic apical blooming appearance of the left ventricle, and this is 4:30 the most 4:31 common and typical form of this disorder. 4:35 There are other variants. 4:36 You can have apical portion of the ventricle being spared, or you can even have 4:42 one segment 4:43 that is affected. 4:46 This is far less common. 4:50 And remember, these ventricular wall motion abnormalities is not a result of 4:56 coronary artery 4:57 disease. 4:59 So the diagnostic criteria for Takatsubo is one, there is no angiographic 5:05 evidence of 5:06 coronary artery disease or acute plaque rupture. 5:10 Two, this is only a transient regional wall motion abnormality, typically with 5:16 no, not 5:17 a single coronary distribution. 5:20 Three, there are new ECG changes with modest troponin elevation, and four, 5:24 there is absence 5:25 of pheochromocytoma or myocarditis. 5:30 Once Takatsubo cardiomyopathy is diagnosed, treatment is largely supportive and 5:34 is similar 5:35 to that for heart failure syndromes, ACE inhibitors, beta blockers, and diure 5:42 tics. 5:42 Most patients will recover cardiac function over the course of a few weeks to 5:47 months. 5:48 As with other forms of new onset heart failure, repeat echocardiography should 5:53 be performed 5:54 in three to six months to evaluate recovery. 5:58 The duration of medical treatment depends on each clinician but typically up to 6:02 one year.