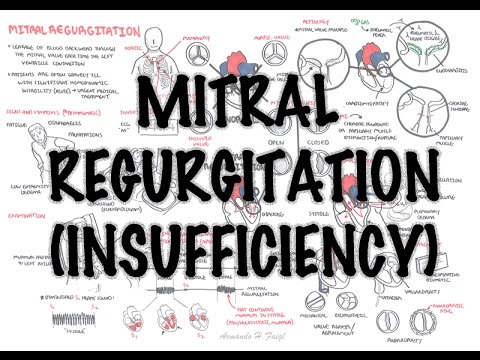
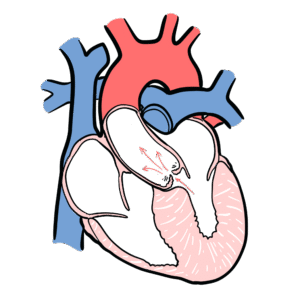
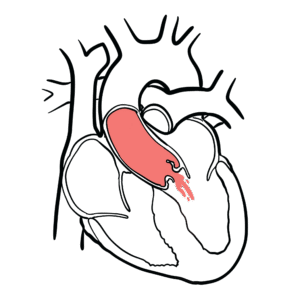
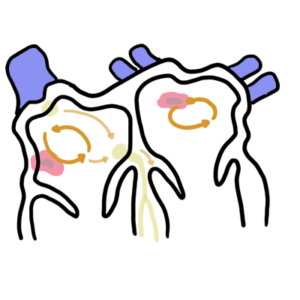
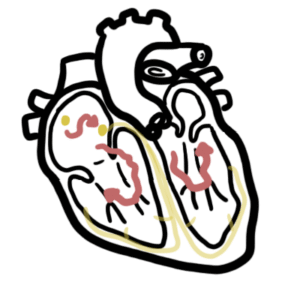
0:00 Mitral valve prolapse is described as bulging of one or more of the mitral 0:12 leaflets into 0:13 the left atrium insistally. 0:16 It is said to be the most common valvular abnormality and is often benign, and 0:21 affecting 0:21 more females. 0:23 Mitral valve prolapse is a cause of mitral regurgitation. 0:27 In men, mitral valve prolapse is likely to progress to significant mitral valve 0:35 regurgitation. 0:36 Let's talk about the normal physiology. 0:39 The mitral valve is a atrial ventricular valve, separating the atria to the 0:45 ventricle. 0:46 The tricuspid valve is also an atrial ventricular valve. 0:50 The mitral valve is made up of two leaflets, and the normal area of the mitral 0:54 valve is 0:55 four to six centimeters squared. 0:59 During diastole, the atria ventricular valves are open, allowing blood to flow 1:04 from the 1:04 atria into the ventricles. 1:10 During ventricular systole, when the heart actually pumps, the mitral valve 1:16 closes, allowing 1:17 blood to be ejected into the aorta and into the rest of the body. 1:24 Let's take a closer look at the mitral valve. 1:28 The mitral valve leaflets lay within the mitral valve annulus, which separates 1:34 the 1:34 left atria to the left ventricle in this specific plane. 1:40 The mitral valve leaflets contain three main layers, atrialis, spongiosa, and 1:49 fibrosa. 1:50 The leaflets are attached to the papillary muscles within the ventricles via 1:56 the caudate 1:57 tendinae. 1:58 During ventricular contraction, the papillary muscles contract to pull on the 2:04 mitral valve 2:05 leaflets via the caudate tendinae to make sure that the mitral valve leaflets 2:12 remain 2:12 closed and not prolapse into the left atria. 2:20 In true mitral valve prolapse, what occurs is that a portion of the mitral 2:26 valve apparatus 2:27 is redundant, and therefore the leaflets they balloon into the left atrium 2:34 during systole. 2:35 Mitral valve prolapse is present if there is more than two millimeter 2:39 displacement of 2:40 the mitral valve leaflets into the left atrium during systole. 2:46 What we see specifically that happens in mitral valve prolapse is that the mit 2:51 ral leaflets 2:52 undergo something called mixometis degeneration, which leads to deposition of 2:58 mucopolysaccharides 3:00 in the middle spongiosa layer of the mitral valve leaflets. 3:05 So what basically happens is that you get deposition within this area and 3:09 therefore proliferation 3:10 of the spongiosa layer resulting in a thickened, stretchy mitral valve leaflets 3:18 and also an 3:19 elongated lax caudate tendinae. 3:22 With a weak leaflet and an elongated caudate tendinae, the mitral valves don't 3:29 shut properly 3:30 during ventricular systoleae and actually prolapse, move into the left atrium. 3:38 And so this can cause a number of problems. 3:42 Complications of mitral valve prolapse include a chordal rupture, the chordet 3:48 endinae rupturing. 3:50 It can cause stagnation within the area, so a thrombus can form, which if 3:57 becomes embolic, 3:58 it can cause a stroke. 4:03 Geocaritis, there can be progression to severe mitral regurgitation, arrhythm 4:09 ias can form 4:10 including atrial fibrillation, and worse sudden death or cardiac neuroses. 4:19 The actual cause for mitral valve prolapse include primary mitral valve prol 4:22 apse, which 4:23 is the most common and really there's no underlying associated diseases, or 4:28 there's secondary 4:29 mitral valve prolapse, which is associated with other conditions, including 4:34 connective 4:34 tissue diseases mainly, mafan syndrome, earless Danlos syndrome, pseudosanthome 4:41 elasticum, osteogenesis 4:43 imperfecta, polycystic kidney disease, and systemic lupus erythmatosis. 4:54 The clinical presentation of mitral valve prolapse is often asymptomatic, 4:59 however one 5:00 can develop palpitations and atypical chest pain, fatigue, dystonia, and 5:07 interestingly 5:07 autonomic dysfunctions, such as anxiety, panic attacks, and syncope. 5:16 On a clinical examination, one can have an irregularly irregular heart rate, 5:21 which would 5:21 indicate atrial fibrillation. 5:24 There can be a displaced apex beat, onosclotation the characteristic murmur is 5:31 a mid to late 5:33 systolic click murmur over the mitral area. 5:40 Certain maneuvers can actually aid in more accurately diagnosing mitral valve 5:44 prolapse 5:45 on examination, so here is a normal heart sound, and here is a mitral valve 6:06 prolapse 6:06 murmur without a maneuver. 6:19 You can appreciate the systolic murmur that occurs mid to late systole with an 6:25 associated 6:25 click. 6:28 Anyway, there are maneuvers that can make this murmur, louder, stronger, 6:37 shorter. 6:38 So a valsava maneuver, which causes a decrease in preload, which means it 6:44 decreases left 6:45 ventricular volume, it will actually produce an earlier and more prominent syst 6:50 olic prolapse 6:52 of the mitral leaflet, causing the systolic click and murmur to move closer to 6:57 S1. 6:57 The first heart sound, and so causes the murmur to become longer. 7:03 Conversely, anything that increases left ventricular volume, such as squatting, 7:09 which will increase 7:10 the preload, it will delay the onset of the click or murmur, and usually dimin 7:15 ishes its 7:16 duration and intensity. 7:20 So to summarize, valsava maneuver will decrease preload, which will therefore 7:26 lengthen the 7:27 murmur, whereas squatting, which will increase preload, will delay and diminish 7:34 the intensity 7:36 of the murmur. 7:38 Other clinical examination findings include pulmonary hypertension. 7:45 Investigations to water include an echocardiogram, which is diagnostic, and can 7:49 assess severity. 7:50 Electrocardiogram can identify possibly atrial fibrillation and may show 7:55 inferior T-wave 7:56 inversion, non-specifically. 8:01 In terms of management, beta blockers are used for symptomatic mitral valve 8:06 prolapse, 8:06 where one has palpitations and chest discomfort. 8:09 However, if complications do emerge, such as severe mitral regurgitation or 8:14 symptomatic 8:15 mitral regurgitation, then obviously other medications are included, and 8:23 possibly mitral 8:23 valve replacement or repair. 8:27 So in summary, mitral valve prolapses when one or two of the leaflets 8:31 essentially prolapse 8:32 into the left atria during systole. 8:36 It's often asymptomatic, however one can develop chest pain and palpitations 8:40 and anxiety-like 8:41 symptoms. 8:42 In that case, beta blockers can be offered. 8:46 The classic murmur is a mid-to-late systolic murmur within associated click.