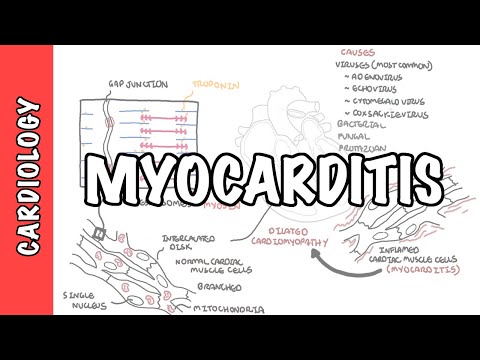
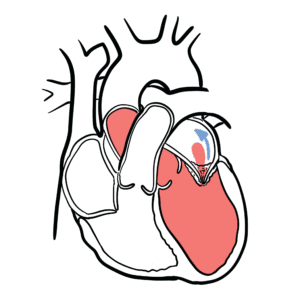
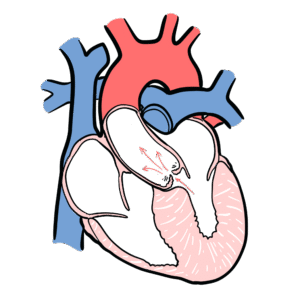
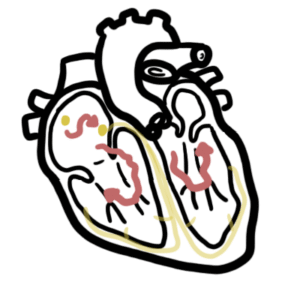
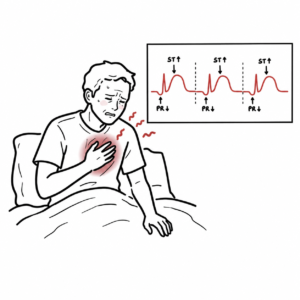
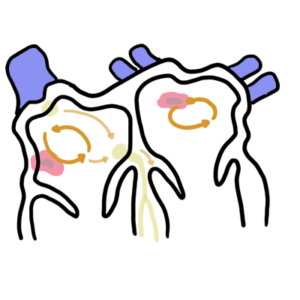
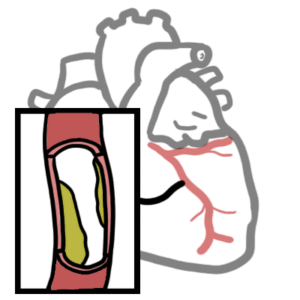
0:00 Cardiomyopathies are diseases of the heart muscle tissue. 0:13 Cardiomyopathies represent a heterogeneous group of diseases that often lead to 0:16 progressive 0:17 heart failure with significant morbidity and mortality. 0:21 When talking about cardiomyopathies, we often focus on ventricular heart 0:26 muscles, the bottom 0:27 two chambers of the heart. 0:29 Remember the heart is a muscular pump, which pumps blood all over our body. 0:33 The cardiac muscle fibers or cells have a single nucleus, they are branched and 0:38 joined 0:39 to one another by intercolated discs. 0:43 The intercolated discs contain gap junctions. 0:46 The intercolated discs and gap junctions form a syncedium of cardiac cells, 0:50 allowing the 0:51 heart to contract in a coordinated unified manner. 0:56 The dismar zones hold the fibers together when the heart contracts, and the 1:01 actual contractile 1:02 units of the cardiac muscles are the sarcomeres, which is made up of myosin and 1:06 actin filaments. 1:08 These two filaments slide past one another to cause a muscle contraction. 1:16 What happens is that the sarcomeres shortens during muscle contraction. 1:21 This is called systole. 1:23 Technology is when the ventricles contract and pumps blood out. 1:29 The sarcomeres lengthens, and this is where the cardiac muscle cells relax. 1:35 The relaxation process is termed diastole. 1:39 This is when the ventricles fill with blood, preparing itself for another 1:44 contraction. 1:46 Because we are focusing on cardiac muscle cells and cardiomyopathies, we need 1:49 to learn 1:49 some fundamental physiology. 1:52 Remember there are three major determinants of myocardial performance, preload, 1:58 afterload 1:59 and contractility. 2:02 Focusing on the ventricular cardiac muscle cells, preload is the amount of 2:05 blood entering 2:06 the ventricles during diastole when the heart is relaxing. 2:11 An increase in preload means a stronger contraction, and this relationship is 2:16 the frank-styling 2:18 relationship which can be depicted with this graph here with di-endistolic 2:23 volume on the 2:24 x-axis, how much blood enters the ventricles, versus stroke volume, which is 2:30 the volume 2:31 of blood ejected by the heart with each contraction. 2:40 To put it simply, as more blood enters the ventricles during diastole, this 2:45 increases 2:46 the length of the resting sarcomere, which builds up tension kind of like a 2:53 spring. 2:54 Tension builds up as the ventricles fill with more blood and then bang during 2:58 systole when 2:59 the sarcomere shortens, it has all this tension and so it just increases the 3:04 contractile force 3:05 and therefore the stroke volume. 3:08 An increase in diastolic volume therefore increases stroke volume normally. 3:15 Preload is the other determinative cardiac muscle function, and this is the 3:19 force the 3:20 cardiomyocytes must overcome to pump blood out of our body. 3:25 Contractility of the heart muscle can be independent of preload, and for 3:29 example the autonomic 3:30 nervous system ions can influence cardiac contractility. 3:38 To finish off this basic anatomy and physiology diagram, you know, troponin is 3:43 attached to 3:44 the structures here and is important and involved in muscle contraction. 3:50 Cardiomyocytes also contain many mitochondria to produce large amounts of ATP 3:55 which is needed 3:56 because the heart muscles always demand this energy, it's constantly pumping. 4:05 Cardiomyopathies as mentioned are diseases of the heart muscle, causing them to 4:09 become 4:10 abnormal enough to lead to heart impairment, and there are many types of cardi 4:15 omyopathies 4:16 but they can be easily or neatly divided into 5 main types based on its anatomy 4:22 and physiology. 4:25 So firstly the most common is dilated cardiomyopathy. 4:29 As the name suggests it is dilatation of the ventricles, dilated ventricles 4:34 make the cardiac 4:35 muscle cells weak and so impairs cardiac contractility and systolic function. 4:43 Second type is hypertrophic cardiomyopathy, and this is where the ventricles 4:49 have hypertrophyid. 4:50 Hypertrophyid typically involves the septum area, the interventricular septum, 4:55 and this 4:56 results in filling issues in the ventricles and so causes a diastolic 5:01 dysfunction and 5:03 is also an important cause of sudden cardiac death in young people. 5:10 Restrictive cardiomyopathy is where the heart muscles become stiff and not 5:15 elastic, they 5:16 are characterized by infiltrative, non-infiltrative, or storage disease is 5:21 causing this restriction, 5:23 this stiffness. 5:25 Restriction of the ventricle means that the sarcomias cannot really lengthen 5:29 effectively 5:30 leading to diastolic problems, so filling problems, and this will obviously 5:34 lead to 5:35 reduced cardiac output. 5:37 The ventricles build pressure in the atria leading to dilated atria. 5:43 The fourth type is one that is not really well known about but it's a rhythm 5:48 ogenic right 5:49 of ventricular cardiomyopathy and this is a problem usually of the right vent 5:55 ricle caused 5:56 by mutation in the desmosone complexes. 6:01 The things remember that hold the cardiac muscle cells together. 6:06 Unclassified cardiomyopathies include things such as peripartum cardiomyopathy, 6:13 tachyarithmia 6:14 induced cardiomyopathy, as well as tachytsubus cardiomyopathy also known as 6:24 broken heart syndrome. 6:25 So each of these five categories or types of cardiomyopathies can be further 6:30 divided 6:30 by the pathogenesis. 6:32 So primary is where the cardiomyopathy is primarily confined to the heart. 6:38 This is usually genetics or inherited cardiac conditions. 6:44 Secondary means that the cardiomyopathy's secondary or occurs as part of 6:50 another systemic 6:51 disorder as a result of toxins or inflammation, infection or other random 7:00 things. 7:01 Cardiomyopathies are diagnosed with echocardiography. 7:05 Some are diagnosed with cardiac MRIs such as infiltrative diseases. 7:10 Other important investigations include chest x-ray which may show signs of 7:13 heart failure, 7:15 opponent which may or may not be elevated, as well as ray-naturtic peptide BNP 7:22 which 7:22 can be elevated if there is a significant component of heart failure. 7:27 Treatment of these cardiomyopathies typically involve heart failure therapies. 7:35 So let us focus on each of these five main classifications of cardiomyopathy in 7:41 more details. 7:43 Please click on the links to learn more about each of these cardiomyopathies.