Otitis Media

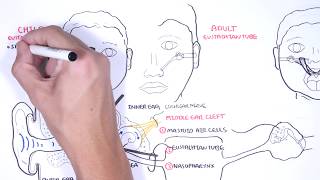
Otitis media (OM) is one of the most common infections in children. OM is inflammation of the middle ear and is usually secondary to bacterial and/or viral infection. It is a complication of eustachian tube dysfunction that occurred during an acute viral upper respiratory tract infection (URTI). The URTI causes effusion in the middle ear which can cause a secondary bacterial infection. The routine prescription of antibiotics in OM is NOT indicated. The overuse of antibiotics may contribute to increasing antimicrobial resistance. Rare complications of AOM include mastoiditis and facial nerve palsy.
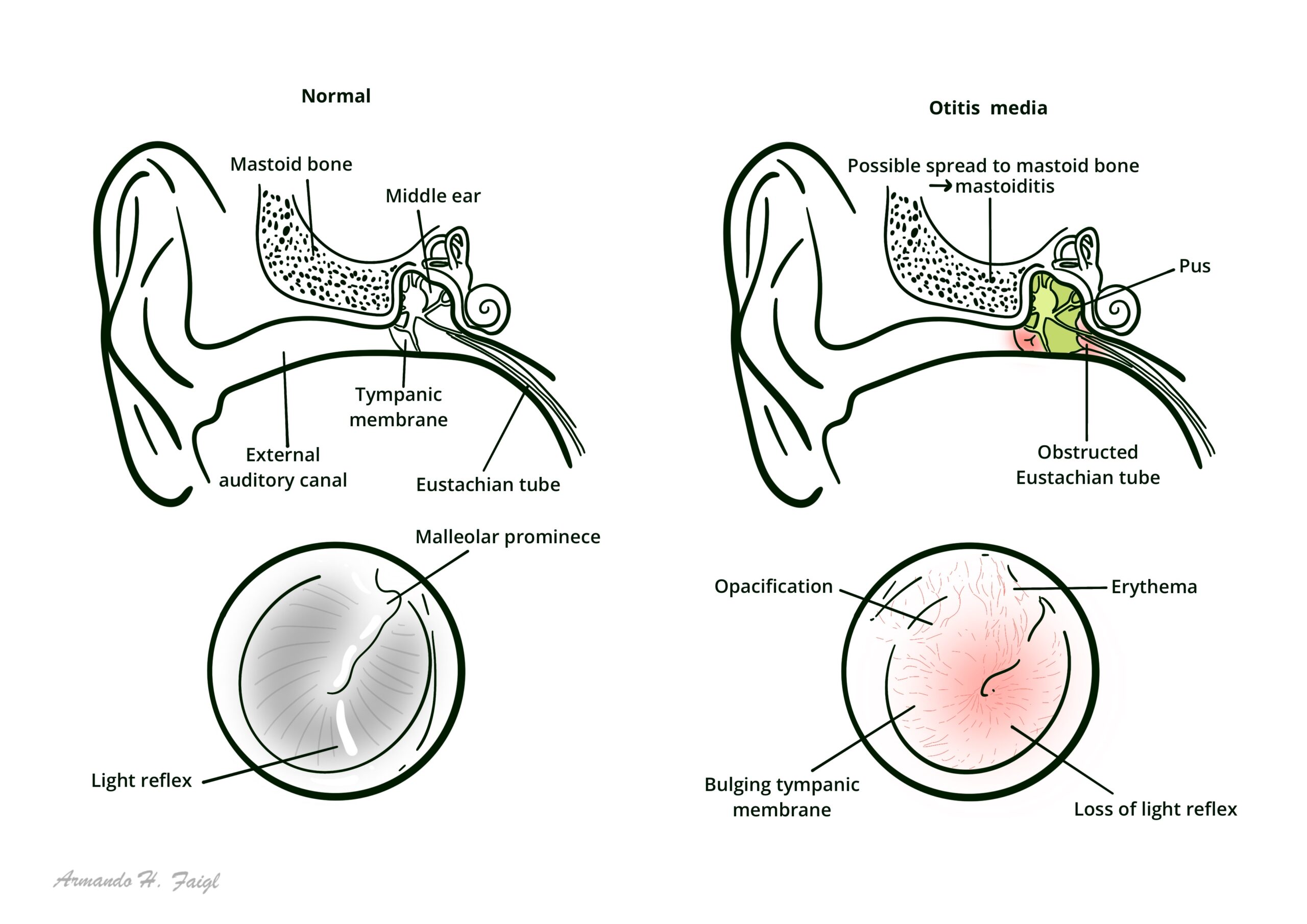
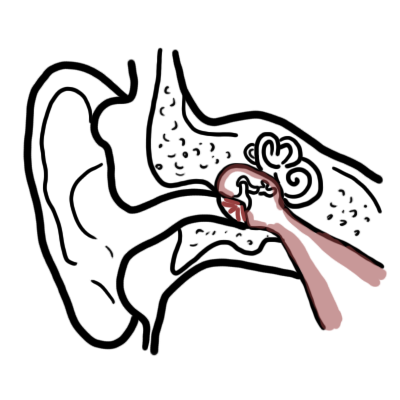
Acute Otitis Media Acute inflammation of the middle ear characterised by otalgia, bulging tympanic membrane and erythema +/- perforation and otorrhoea
Otitis Media with effusion (Glue Ear): Also known as serous otitis media characterised by fluid in the middle with without symptoms or sign of acute inflammation of ear.
Recurrent Acute Otitis Media: Is three episodes of AOM within a six month period.
Suppurative Otitis Media: Persistent inflammatory process associated with a perforated tympanic membrane and pus draining from the ear.
Otitis externa: Inflammation of the outer ear canal, often due to bacterial or fungal/ yeast infection. Otitis externa may occur in isolation, or can be associated with AOM and perforation of the tympanic membrane.
Epidemiology
A child with otitis media can also have serious bacterial infection such as septicaemia or meningitis. If systemically unwell, consider coexistent causes of sepsis.
Acute Otitis Media – Acute inflammation of the middle ear
Otitis Media with effusion – Also known as serous otitis media characterised by fluid in the middle with without symptoms or sign of acute inflammation of ear. Can be discovered during routine audiometric screening.
Chronic suppurative otitis media
Bedside
Other
Chronic suppurative otitis media is a common cause of hearing impairment, disability, and poor scholastic performance. Occasionally it can lead to fatal intracranial infections and acute mastoiditis, especially in developing countries.
Acute Otitis Media (AOM)
Children diagnosed with AOM should not routinely be prescribed antibiotics. Exceptions exist for high risk groups and persistent infection.
Children with AOM should not be prescribed decongestants or antihistamines.
Otitis Media with Effusion (OME)
Tympanostomy tubes (grommets) help fluid drain from the middle ear by decreasing pressure in the middle ear. Fluid also can flow into the nose via eustachian tube.
| Refer to ENT specialist |
| OME for three months or more with evidence of hearing loss or retraction of the tympanic membrane. |
| Recurrent AOM |
| Serious complications of AOM such as mastoiditis or facial nerve paralysis |
| Patients with a high risk of OME, such as those with craniofacial abnormalities e.g. Down syndrome and cleft palate |
| Discharge with cholesteatoma or chronic suppurative otitis media |
Mastoiditis Osteomyelitis of the mastoid bone (mastoiditis) is a complication of AOM. Characterised by post auricular swelling and redness. Computed Tomography (CT) scan shows bony destruction of mastoid air cells.
Chronic suppurative otitis media is persistent inflammation of the middle ear or mastoid cavity. Synonyms include chronic otitis media, chronic mastoiditis, and chronic tympanomastoiditis. Chronic suppurative otitis media is characterized by recurrent or persistent ear discharge (otorrhea) over two to six weeks through a perforation of the tympanic membrane. Chronic suppurative otitis media usually begins as a complication of persistent AOM with perforation in childhood. Typical findings may also include thickened granular middle ear mucosa and mucosal polyps. Occasionally, chronic suppurative otitis media will be associated with a cholesteatoma within the middle ear. Chronic suppurative otitis media is differentiated from chronic otitis media with effusion, in which there is an intact tympanic membrane with fluid in the middle ear but no active infection. Chronic suppurative otitis media does not include chronic perforations of the eardrum that are dry, or that only occasionally produce discharge, and have no signs of active infection.
Overview
Cholesteatoma is a locally destructive lesion of the middle ear, in the form of a cyst of keratinous epithelium. Cholesteatoma can occasionally lead to serious consequences, including facial palsy, meningitis, or brain abscess. It should be suspected in any case of persistent or recurrent ear discharge. The key to diagnosis is a characteristic appearance on otoscopy.
Investigation
Aetiology is debated, but cholesteatoma probably arises from the lateral epithelium of the tympanic membrane, and then grows as a self perpetuating mass into the middle ear.
Complications
Remember it is a growing mass.
References
Bhutta, MF. (2011). Cholesteatoma. British Medical Journal










Discussion