

Chest Trauma

Overview
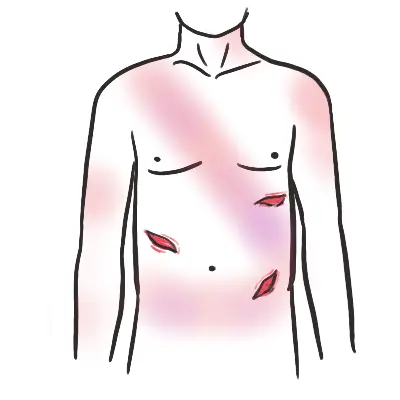
Thoracic trauma causes injuries to the chest wall, lungs, great vessels, and heart. It is clinically divided into blunt and penetrating injuries.
- Blunt Thoracic Injuries
- Pneumothorax
- Flail chest
- Aortic injury
- Myocardial Injury
- Pulmonary contusion
- Penetrating Injuries
- Tension Pneumothorax
- Open Pneumothorax
- Haemothorax
- Cardiac tamponade
PAMD
- Preparation
- Assessment – Primary Survey
- Management
- Assessment – Secondary Survey
- Dislocation
Preparation
- Staff
- Equipment
Assessment – Primary Survey – ABCDE
- Airway – Patent and Protected
- Foreign bodies
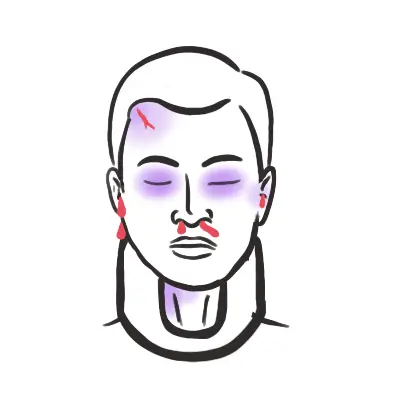
- Facial, mandibular, or tracheal/laryngeal fractures
- Management
- Insertion of nasogastric tube important to minimise likelihood of aspiration
- Ensure oxygen delivery to brain through intubation and prevent hypercarbia
- Intubate if GCS < 9, patient is hypoxic, injury at or above C4
If the patient is able to communicate verbally, the airway is usually patent.
- Breathing – Look, listen, feel
- Oxygen saturation
- Identify any life-threatening conditions affecting thorax
- Tension pneumothorax – deviated trachea?
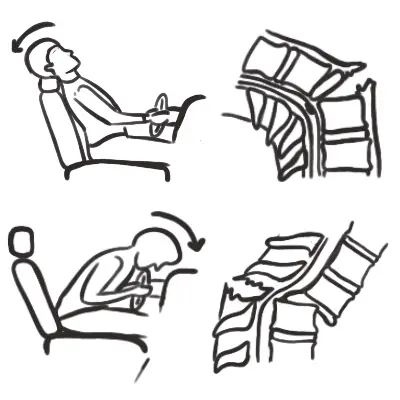
- Flail Chest – Paradoxical movement of chest wall segment
- Consider diaphragm issues (injury at C3, C4, C5)
- Watch for respiratory insufficiency
- In the absence of major airway obstruction and flail chest, the presence of paradoxical breathing is considered highly suggestive of cervical spine injury
- Management
- High flow oxygen
Ventilation may be reduced for a number of reasons, (1) diaphragm fatigue, (2) Progressively ascending spinal cord damage from primary damage or secondary ascending spinal cord oedema encroaching on C3-C5, (3) These same segments may be involved from primary injury and diaphragm may be partially paralysed and (4) Consequence of co-existing chest trauma.
- Circulation
- HR, BP, Capillary refill, skin colour
- Distended neck vein – Cardiac tamponade?
- Auscultate for murmur – Pericardial friction rub?
- Asymmetric pulses – aortic problems
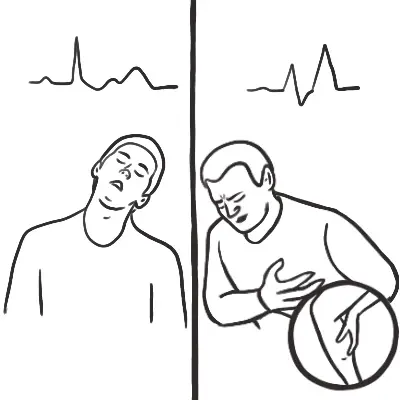
- Look for signs of shock or unstable rhythm
- Hypotensive trauma victims should be considered as intravascularly volume depleted and bleeding until proven otherwise
- Look for signs of shock or unstable rhythm
- If hypotensive – IV fluids
- Disability
- GCS
- Pupils – equal and reactive
- Neurological examination – motor, sensory, reflex
- Suspect C-spine injury until ruled out
- Check Bulbocavernosus reflex – negative sign suggests complete spinal cord injury
- Spinal immobilisation until spinal cord or unstable vertebral injury has been excluded on physical examination and investigations
- Exposure/Environment
- Increased risk of hyperthermia due to peripheral vasodilation
- Look for other injuries
- Fractures – Basilar skull fracture?
- Scalp laceration
- Burns
- Management
- Warm IV fluids
- Warm blankets
| INVESTIGATIONS | ||
| Bedside | Laboratory | Imaging |
| ECG | FBC | X-Ray – Neck, Thorax, Pelvis |
| Ultrasound (FAST)? | EUC | Head CT scan (non-contrast) |
| Blood glucose | Cross match | Chest CT |
| Urinalysis | ||
| Serum lactate | ||
Assessment – Secondary Survey (Head to Toe)
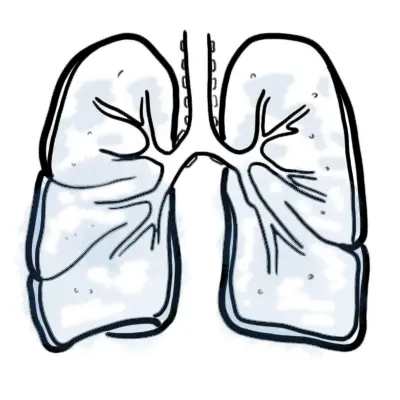
Pneumothorax The abnormal presence of air in the pleural cavity. The air inside the pleural cavity separating the visceral from the parietal pleura, with subsequent collapse of the adjacent lung, is known as pneumothorax.
As alluded to above, air does not normally exist within the pleural space. The pressure within the pleural space is negative with respect to the alveolar pressure during the entire respiratory cycle.
Classification
The causes of Pneumothorax can be divided into three Groups: Primary Spontaneous Pneumothorax, Secondary spontaneous pneumothorax and traumatic pneumothorax.
- Primary spon. pneumothorax occurs spontaneously without evidence of lung disease. More common in tall skinny people especially young males who are also smoker. 10-30yo. What happens is that air escapes from the lung into the pleural space through rupture of a pleural bleb, no evidence of hole in the parietal pleura.
- A pulmonary bleb is a small collection of air between the lung and the outer surface of the lung (visceral pleura) usually found in the upper lobe of the lung.
- When a bleb ruptures the air escapes into the chest cavity causing a pneumothorax (air between the lung and chest cavity) which can result in a collapsed lung. Primary spon. pneumothorax can reoccur. 50% of the time on the same side. 10% of the time on the opposite side.
- Secondary Spon Pneumothorax is a more serious event than a primary pneumothorax. Because, by definition, the patient has underlying lung disease. A pneumothorax in a patient with already diminished pulmonary reserve can be life-threatening and requires more immediate medical attention and intervention. SSP can be caused by COPD, asthma, cystic fibrosis, interstitial lung disease. In these people the cause is typically a bulla. If blebs become larger or come together to form a larger cyst, they are called bulla, which then can rupture into the pleural cavity.
- Traumatic pneumothorax Trauma is the most common cause of pneumothorax secondary to a penetrating (eg, knife) or blunt (eg, rib fracture) mechanism. Injury to the rib cage can cause a hole in the parietal pleura allowing air to enter from the outside to the pleural cavity. Trauma can also injury the lung tissue potentially injuring the visceral pleura, again allowing entry of air from the pulmonary tree into the pleural cavity.
If you wanna drop some big concepts you can talk about subcutaneous emphysema. This is where gas/air escapes from the lungs and become trapped in the subcutaneous tissue below the skin. This is often cause following trauma, but can also occur spontaneously. From a punctured lung the air will travel to the mediastinum from which it Air is able to travel to the soft tissues of the neck and the retroperitoneum (the space behind the abdominal cavity) because these areas are connected by fascial planes.
Types of Pneumothorax there is open, close or tension. PSP and SSP usually causes closed pneumothorax. Traumatic usually causes Closed pneumothorax. We will talk about tension later because it s a big deal.
- In open Pneumothorax the pleural cavity is open to the environment because of some form of trauma damaging the parietal pleura. Breathing in allows air into the pleural cavity, breathing out allows air to exit the pleural cavity. Therefore the pleural cavity pressure is the same as the atmospheric pressure.
- In closed Pneumothorax there is air in the pleural cavity because of air coming in from the lungs due to a potential defect or hole in the visceral pleura. The parietal pleura is sealed. Inspiration, breathing in, brings air inside the pleural cavity. This means that initially the pleural cavity pressure will be less then the atmospheric pressure, because air moves into the pleural cavity. Possibly, Air keeps coming inside the pleural cavity until it stabilizes then the pressure becomes equal
The treatment for simple pneumothorax depends if it is a small or a big pneumothorax. If it is a small pneumothorax these are allowed to resolve spontaneously and may be treated with 100% O2 by face mask. Large, severely symptomatic pneumothoraces are treated with a chest tube and/or pleurodesis.
Small pneumothorax can be treated because air in the pleural cavity the air we breath in is predominately nitrogen. By giving a person 100% oxygen, you decrease the partial pressure of nitrogen in the persons blood, thereby establishing a diffusion gradient (nitrogen moves into blood). If course you create an O2 diffusion gradient too, but O2 diffuses more slowly and is absorbed by surrounding tissue for energy.
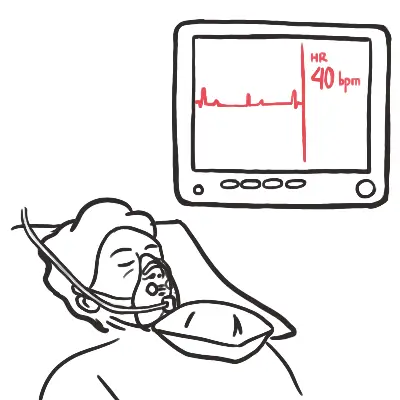
Most patients present with unilateral pleuritic chest pain and dyspnoea. Classical physical signs may not be present (depending upon the size of the pneumothorax): tachypnea , tachycardia, normal/hyper-resonant percussion note because of air in the cavity, decrease air entry on the affected side because of poor filling. Rarely, there may be a clicking sound at the cardiac apex.
But both open and close can lead to tension pneumothorax
- Tension pneumothorax is life-threatening and there should be no delay in treatment. Tension pneumothorax is there is air in the pleural cavity, but the air here is so much, it increases the pressure in the pleural cavity a lot to cause compression of surrounding structures.
- This deadly variant of pneumothorax occurs because of a pulmonary or chest wall defect that acts as a one-way valve, drawing air into the pleural space during inspiration but trapping it during expiration.
- The pleural cavity pressure is greater than the atmospheric pressure.
- Etiologies include penetrating trauma, infection, CHF, and positive-pressure mechanical ventilation. The pathophysiology of tension pneumothorax involves the following:
- As mentioned an open of closed pneumothorax can cause a tension. Essentially, the ipsilateral lung collapse 2° to an ↑amount of trapped air on the affected side. This increase in air, increase in pressure in the affected side pushes the mediastinum away from towards the unaffected side causing Tracheal Deviated because of the pressure on one side pushing against the trachea. Respirator distress due to the obstruction caused by tracheal deviation and poor oxygen flow into the lungs. Therefore you can get decrease in O2 saturation. The heart can be pushed causing Impaired venous return leading to ↓cardiac output and therefore hypotension. The impaired venous return can also mean that blood will pool back causing distention of the neck veins. Shock and death occur unless the condition is immediately recognized and treated.
- Tension pneumothorax requires immediate needle decompression with a needle usually 2nd intercostal space mid clavicular. Once decompression is achieved, a chest tube (thoracostomy tube) can be placed. Administer IV fuids to ↑ venous return to the heart.
Flail Chest
Overview
Flail chest occurs when a segment of the rib cage breaks under extreme stress and becomes detached from the rest of the chest wall. The definition is actually complex. Production of a flail segment of chest wall requires multiple rib fractures.
- Definition
- The rib fractures specifically are double fractures of three or more contiguous ribs.
- Combined sternal and rib fractures, to uncouple the segment from the surrounding chest wall.
- Obviously something traumatic has to cause fracture to the ribs. Such as a MVA (80%), then there is falls especially in the elderly, and the third is blunt trauma especially those with genetic condition such as osteogenesis imperfect.
- The so called flail segment of the rib now will move paradoxiacally with the other chest wall. Because when you think about it, it its now basically part of the lungs.
Management
The basic objective of treatment is to control pain and minimize atelectasis. Improved pain control also would enhance cough efficiency and allow for larger tidal volumes and reduce dead space ventilation.
- More fractures more complications
- Monitoring
- Pain control
- Mechanical ventilation (Invasive ventilation)
- Chest physiotherapy
Complications
- Pneumonia
- Pneumothorax
- Haemothorax
- Pulmonary contusion
- Aortic injury
- Pain and disability
- Pulmonary emoblism







Members only discussions coming soon…