

Head and Brain Trauma
Overview
- Traumatic Brain Injury – classified as mild, moderate or severe based on GCS
- Concussion
- Cerebral contusion (intracerebral haemotoma)
- Subarachnoid Haemorrhage
- Subdural Haemorrhage
- Epidural Haemorrhage
- Diffuse axonal Injury
PAMD
- Preparation
- Assessment – Primary Survey
- Management
- Assessment – Secondary Survey
- Dislocation
Preparation
- Staff
- Equipment

Assessment – Primary Survey – ABCDE
- Airway – Patent and Protected
- Foreign bodies
- Facial, mandibular, or tracheal/laryngeal fractures
If the patient is able to communicate verbally, the airway is usually patent.
- Breathing – Look, listen, feel
- Identify any life-threatening conditions affecting thorax
- Tension pneumothorax
- Flail Chest
- Identify any life-threatening conditions affecting thorax
Ventilation may be reduced for a number of reasons, (1) diaphragm fatigue, (2) Progressively ascending spinal cord damage from primary damage or secondary ascending spinal cord oedema encroaching on C3-C5, (3) These same segments may be involved from primary injury and diaphragm may be partially paralysed and (4) Consequence of co-existing chest trauma.
- Circulation
- HR, BP, Capillary refill, skin colour
- Look for signs of shock or unstable rhythm
- Hypotensive trauma victims should be considered as intravascularly volume depleted and bleeding until proven otherwise
- Disability
- GCS
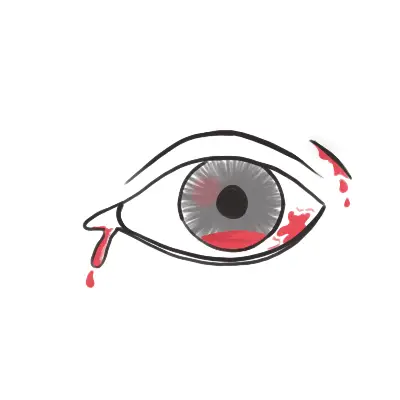
- Pupils – equal and reactive
- Neurological examination – motor and sensory
- Suspect C-spine injury until ruled out
- Check for signs of ↑ICP – Cushing’s response (bradycardia, hypertension, irregular respirations)
A dilated pupil in an unconscious patient with head trauma is evidence of transtentorial herniation caused by downward pressure on the uncus and ipsilateral 3rd cranial nerve.
- Exposure/Environment
- Increased risk of hyperthermia due to peripheral vasodilation
- Look for other injuries
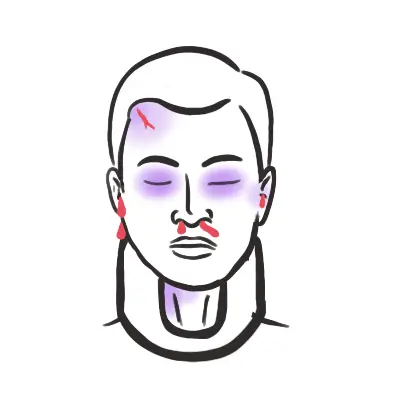
- Fractures – Basilar skull fracture?
- Scalp laceration
- Burns
| Warning Signs of Severe Head Injury |
| GCS <8 |
| Deteriorating GCS |
| Unequal pupils |
| Lateralizing signs |
| INVESTIGATIONS | |
| Laboratory | Imaging |
| FBC | X-Ray – Neck, Thorax, Pelvis |
| EUC | Head CT scan (non-contrast) |
| Cross match | Ultrasound (FAST)? |
| Urinalysis | MRI – axonal injury is suspected |
| Pregnancy test | Angiogram? |
| Serum lactate | |
| Glucose | |
Management-The aim is to reduce secondary brain injury
- Airway – Patent and Protected
- Insertion of nasogastric tube important to minimise likelihood of aspiration
- Ensure oxygen delivery to brain through intubation and prevent hypercarbia
- Intubate if GCS < 9, patient is hypoxic, injury at or above C4′
- Oxygen!
Avoid secondary brain injury by preventing hypotension, hypoxia, fever, seizures and hyperglycaemia.
- Breathing – Look, listen, feel
- Consider diaphragm issues (injury at C3, C4, C5)
- Identify and treat life threatening chest injury
- In the absence of major airway obstruction and flail chest, the presence of paradoxical breathing is considered highly suggestive of cervical spine injury
- Circulation
- Disability
- GCS
- Pupils – equal and reactive
- Neurological examination – motor and sensory
- Spinal immobilisation until spinal cord or unstable vertebral injury has been excluded on physical examination and investigations (using nexus criteria as an example)
- If signs of increased intracranial pressure
- Calm (sedate) if risk for high airway pressures or agitation – paralyze if agitated
- Elevate head of bed
- Hyperventilate (100% O2) to a pCO2 of 30-35 mmHg
- Adequate BP to ensure good cerebral perfusion
- Mannitol 1g/kg infused rapidly (contraindicated in shock/renal failure
- Surgical – decompression, drainage
for raised ICP make sure to control perfusion, glucose, temperature and seizures.
- Exposure/Environment
- Increased risk of hyperthermia due to peripheral vasodilation
- Warm IV fluids
- Warm blankets
- Look for other injuries
- Increased risk of hyperthermia due to peripheral vasodilation
Consult the neurosurgeon early and aggressively treat hypoxia, hypotension, herniation, and seizures to avoid secondary (preventable) injuries.
Early and Late signs of Head trauma
Assessment – Secondary Survey (Head to Toe) – Once patient is stabilised








Members only discussions coming soon…