

Notes »
clinical
» Neurology
Cerebellar Presentation
Overview
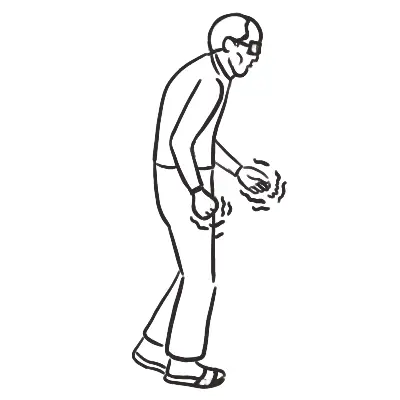
Signs and symptoms of cerebellar disease presents on the same side (ipsilateral). Symptoms and signs consist of gait impairment, unclear (“scanning”) speech, visual blurring due to nystagmus, hand in-coordination, and tremor with movement.
| Remember |
| CAUSES OF CEREBELLAR DISEASE BASED ON ONSET | ||
| Acute | Subacute | Chronic |
| Drugs (phenytoin, lithium) | Alcohol | Chronic infection |
| Alcohol intoxication | Malnutrition (Vitamin B12 and B1 deficiency | Friederichs ataxia |
| Paraneoplastic syndrome | Hypothyroidism | |
| Hyponaturaemia | ||
| CAUSES OF CEREBALLAR DISEASE BASED ON LOCATION | |||
| Unilateral | Bilateral | Midline | Vermis |
| Space occupying lesion | Drugs (phenytoin) | Paraneoplastic Syndrome | Alcohol |
| Ischaemia | Alcohol | ||
| Multiple sclerosis | Friederichs ataxia | ||
| Trauma | Hypothyroidism | ||
| Large space occupying lesion | |||
| Multiple Sclerosis | |||
| Trauma | |||
| Frederichs ataxia is a autosomal recessive ataxia, comprising one-half of all hereditary ataxias. Two forms classic (frataxin) and association with vitamin E deficiency. |
Cerebellar Examination
General
- Titubation
- Gait - ataxia, unable to tanden gait (heel to shin)
- Intention tremor
Head
- Auscultate over cerebellum for bruits
- Auscultate carotids - lateral medullary syndrome (Wallenburg syndrome)
- Cerebellopontine angle tumour - 5, 7, 8 cranial nerve affected
- Nystagmus
- Speech - explosive, jerky and loud with irregular seperation of syllables
Arms and legs
- Shake hands - tone
- Upward arm drift (due to hypotonia of the agonist muscles)
- Rebound - ask patient to raise arm quickly and stop (incoordination between antagonist and agonist muscles)
- Hypotonia - due to loss of facilitatory muscles
- Coordination
- Finger to nose - past pointing due to no connection between brainstem and cerebellum
- Heel-to-shin
- Dysdiadochokinesis - inability to perform rapid alternating movements
Special tests
- Trunkal ataxia (usually assocated with vermis pathology of the cerebellum)
- Reflex - pendular knee
| Side note There are many connections between the cerebellum and the parietal and frontal lobes of the brain and thus explains the clinical presentation that is associated with cerebellar disease. |
Pathways in the CNS
Pyramidal Pathways (through medulla)
- Anteriorcorticospinal tract
- Lateralcorticospinal tract
Extrapyramidal Pathways
- Rubrospinal tract
- Vestibulospinal tract
- Reticulospinal tract
- Tectospinal tract
- Olivospinal tract
Cerebellar Pathway
- Spinocerebellar tract
| CLINICAL DIFFERENCES BETWEEN THE CENTRAL NERVOUS SYSTEM PATHWAYS | ||||
| Clinical signs | Pyramidal | Extrapyramidal | Cerebellar | Functional |
| Power | Weak | No weakness | No weakness | Give-way weakness |
| Wasting | None (overtime no use maybe) | None | None | None |
| Tone | Spastic increase | Rigidity | Normal/reduced | Normal |
| Reflexes | Increased | Normal | Normal | Normal |
| Plantar response | Extensor | Flexor | Flexor | Normal |
| Coordination | Reduced by weakness | Normal but slow | Impaired | Normal (laborious) |
Related conent
Related posts

Latest posts




Discussion
Login/Signup
High quality discussions coming soon
0 Comments
Most Voted