

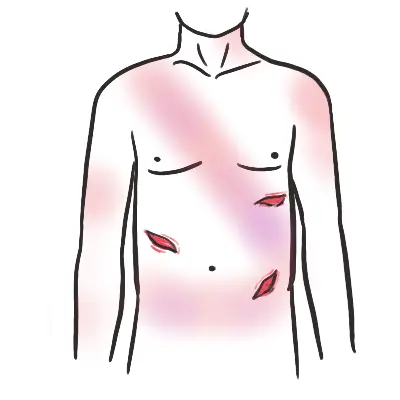
Abdominal Trauma
Overview
Abdominal trauma can result in injuries that are intraperitoneal and retroperitoneal
- Retroperitoneal organs
- Kidneys
- GU tract
- Duodenum
- Pancreas.
- Intraperitoneal injuries occur to the solid and hollow organs and the diaphragm.
Abdominal trauma is divided into blunt and penetrating mechanisms. Blunt abdominal trauma involves a crushing force that causes disruption of solid viscera (spleen or liver) or hollow viscera (intestine). These injuries are most common after falls or MVCs. Penetrating abdominal trauma occurs most commonly due to stab wounds and gunshot wounds that enter the intraperitoneal cavity.
- Blunt Thoracic Injuries
- Splenic laceration
- Liver laceration
- Pancreatic injury
- Bowel perforation
- Duodenal haematoma
- Diaphragmatic injury
- Retropertioneal haemotoma
- GU injury
- Penetrating Injuries
- Any organ
PAMAD
- Preparation
- Assessment – Primary Survey
- Management
- Assessment – Secondary Survey
- Dislocation
Preparation
- Staff
- Equipment
Assessment – Primary Survey – ABCDE
- Airway – Patent and Protected
- Foreign bodies
- Facial, mandibular, or tracheal/laryngeal fractures
- Management
- Insertion of nasogastric tube important to minimise likelihood of aspiration
- Ensure oxygen delivery to brain through intubation and prevent hypercarbia
- Intubate if GCS < 9, patient is hypoxic, injury at or above C4
If the patient is able to communicate verbally, the airway is usually patent.
- Breathing – Look, listen, feel
- Oxygen saturation
- Identify any life-threatening conditions affecting thorax
- Tension pneumothorax – deviated trachea?
- Flail Chest – Paradoxical movement of chest wall segment
- Consider diaphragm issues (injury at C3, C4, C5)
- Watch for respiratory insufficiency
- In the absence of major airway obstruction and flail chest, the presence of paradoxical breathing is considered highly suggestive of cervical spine injury
- Management
- High flow oxygen
Ventilation may be reduced for a number of reasons, (1) diaphragm fatigue, (2) Progressively ascending spinal cord damage from primary damage or secondary ascending spinal cord oedema encroaching on C3-C5, (3) These same segments may be involved from primary injury and diaphragm may be partially paralysed and (4) Consequence of co-existing chest trauma.
- Circulation
- HR, BP, Capillary refill, skin colour
- Distended neck vein – Cardiac tamponade?
- Auscultate for murmur – Pericardial friction rub?
- Asymmetric pulses – aortic problems
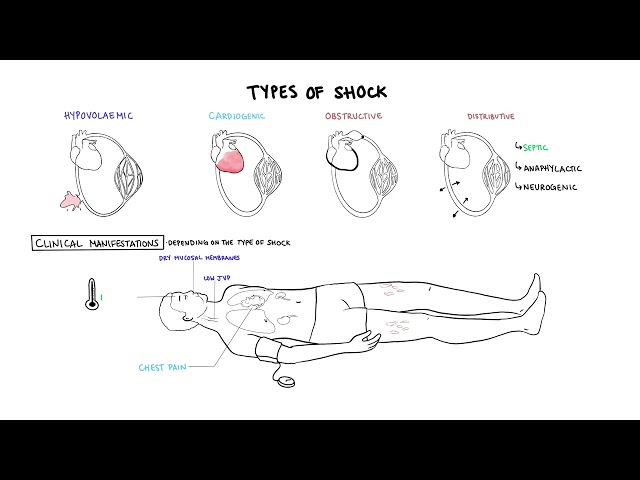
- Look for signs of shock or unstable rhythm
- Hypotensive trauma victims should be considered as intravascularly volume depleted and bleeding until proven otherwise
- Look for signs of shock or unstable rhythm
- Management
- 2 large IV insertion
- Cross match
- If hypotensive – IV fluids
- Rule our haemorrhagic and maintain MAP >65 with vasoconstrictors
- Disability
- GCS
- Pupils – equal and reactive
- Neurological examination – motor, sensory, reflex
- Suspect C-spine injury until ruled out
- Management
- Check Bulbocavernosus reflex – negative sign suggests complete spinal cord injury
- Spinal immobilisation until spinal cord or unstable vertebral injury has been excluded on physical examination and investigations
Kehr’s sign Pain in the shoulder that is not associated with tenderness or pain with shoulder ROM suggests that blood is present under the diaphragm, causing referred pain to the shoulder. This commonly occurs from a splenic or liver laceration.
- Exposure/Environment
- Increased risk of hyperthermia due to peripheral vasodilation
- Look for other injuries
- Fractures – Basilar skull fracture?
- Scalp laceration
- Burns
- Management
- Warm IV fluids
- Warm blankets
| INVESTIGATIONS | ||
| Bedside | Laboratory | Imaging |
| FAST scan | FBC | X-Ray – Neck, Thorax, Pelvis |
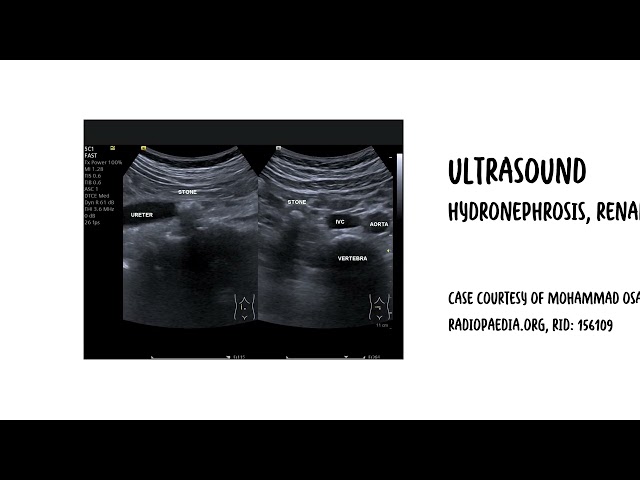
| Urinalysis | EUC | Abdominal CT scan |
| Blood glucose | Cross match | Chest CT |
| VBG | Urinalysis | Ultrasound (FAST)? |
| ECG | Serum lactate | MRI – ligament injury suspected |
| FAST SCAN |
| Perihepatic & hepato-renal space – Pouch of Rutherford-Morison |
| Perisplenic |
| Pelvis – Pouch of Douglas |
| Pericardium |








Members only discussions coming soon…