

Acute Kidney Injury (AKI)
Overview
Acute Kidney Injury (AKI) and Acute Kidney Disease (AKD) describe a spectrum of sudden decline in renal function occurring over hours to days, characterized by a rapid drop in glomerular filtration rate (GFR), accumulation of nitrogenous waste products (azotemia), and deregulation of extracellular fluid volume and electrolytes. Under the KDIGO framework, AKI represents acute deterioration occurring within 7 days, whereas AKD encompasses acute or ongoing kidney injury and/or dysfunction lasting up to 90 days (after which it is officially classified as Chronic Kidney Disease).
Epidemiologically, AKI is extremely common, affecting approximately 10–15% of all hospitalized patients and over 50% of patients admitted to intensive care units (ICU). The incidence has risen steadily due to an aging population, increasing prevalence of chronic comorbidities (such as diabetes, heart failure, and pre-existing CKD), and frequent exposure to nephrotoxic medications or diagnostic procedures. AKI carries substantial short-term morbidity and mortality, particularly when severe enough to require renal replacement therapy, and serves as a major independent risk factor for the future development of CKD and end-stage renal disease.
AKI is neither a diagnosis nor a disease. Rather, it is a clinical syndrome that is caused by, or complicates, a wide range of disorders
Definition
KDIGO Criteria: Standardized diagnostic definition of AKI based on an increase in serum creatinine by >= 0.3 mg/dL (>= 26.5 umol/L) within 48 hours, or an increase to >= 1.5 times baseline within 7 days, or urine output < 0.5 mL/kg/hr for 6 consecutive hours.
Acute Kidney Disease (AKD): Acute or ongoing kidney injury and/or reduced function (GFR < 60 mL/min/1.73m2 or marker of kidney damage) lasting between 7 days and 90 days post-AKI onset.
Azotemia: Accumulation of nitrogenous waste products (blood urea nitrogen and serum creatinine) in the blood due to decreased GFR; becomes clinical “Uremia” when accompanied by systemic symptoms.
Fractional Excretion of Sodium (FENa): Percentage of sodium filtered by the glomerulus that is excreted in urine; used to differentiate prerenal azotemia (< 1%) from intrinsic renal injury (> 2%).
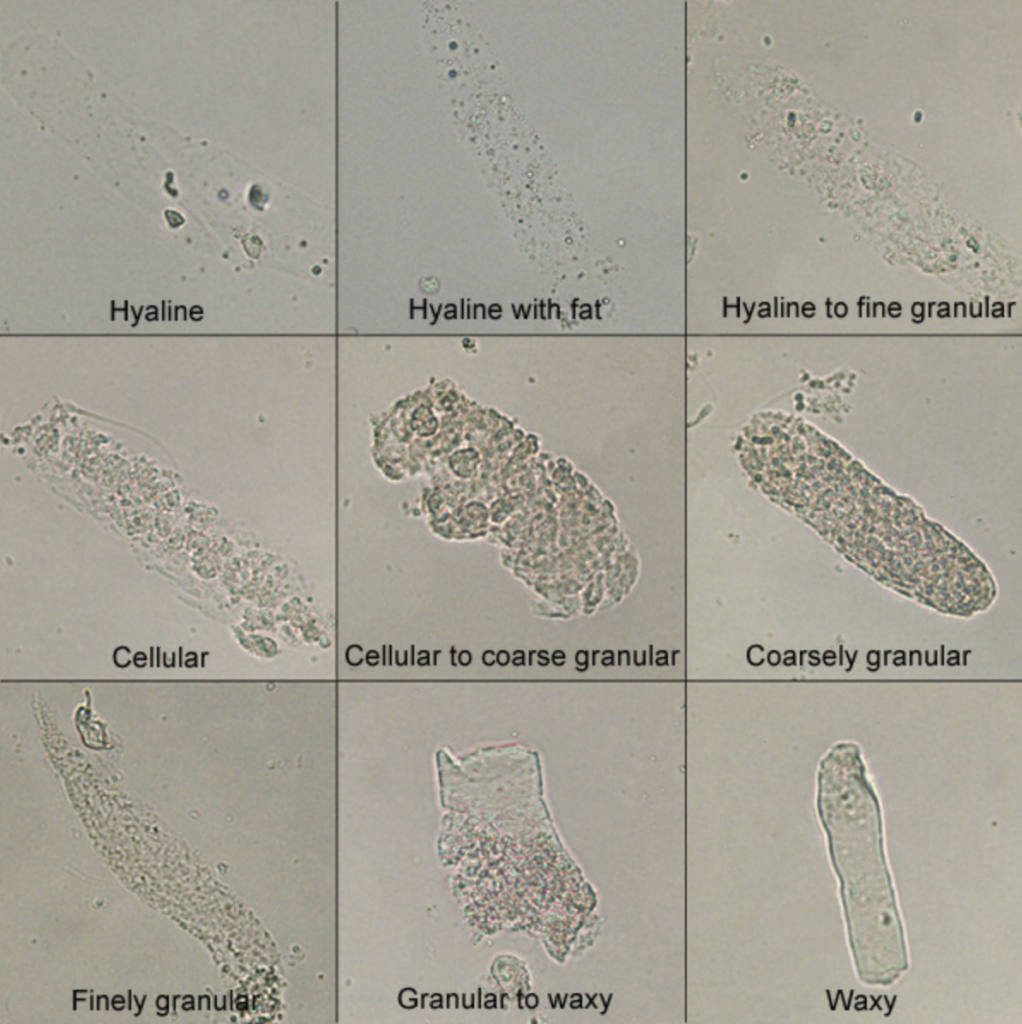
Muddy Brown Granular Casts: Sloughed tubular epithelial cell aggregates pathognomonic for Acute Tubular Necrosis (ATN)
Anatomy and Physiology
Renal Anatomy
The urinary system consists of:
- Kidneys
- Ureters
- Bladder
- Urethra
The kidneys are retroperitoneal bean shaped organs thats sits between veretbral levels T11-L3, the left kidney sitting slightly higher then the right kidney.
The kidneys is divided into three sections:
- Renal cortex – renal arches and renal columns
- Renal Medulla – pyramids, papillae, major calyx, minor calyx
- Renal Sinus – Pelvis, renal vessels and lymphatics
Arterial Supply
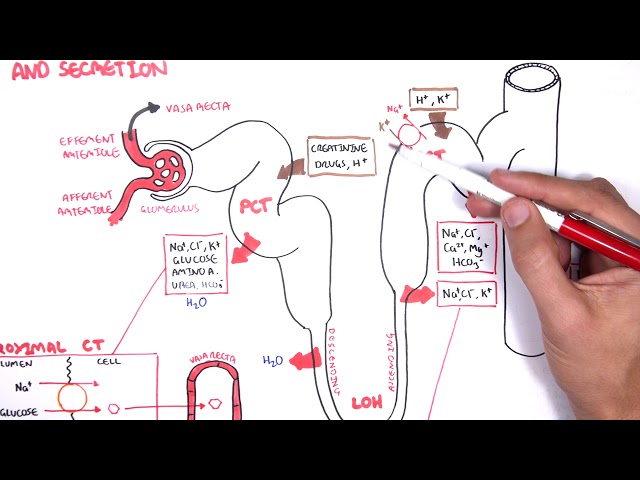
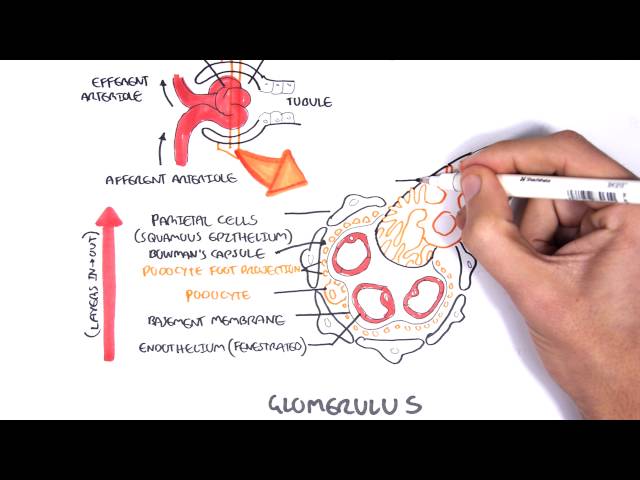
- Aorta → Renal artery (L2) → Segmental artery → Interlobular artery → Cortical radiate artery → Afferent Arteriole → GLOMERULUS
Venous Drainage
- GLOMERULUS → Efferent arteriole (has branches forming the Vasa recta) → Arcuate vein → Interlobar vein → Renal Vein → Inferior vena cava
Nephrons
- Functional units of Kidneys
- Nephron’s are structurally divided into two types:
- Cortical
- Juxtamedullary
Ureters are narrow muscular tube that transport urine to the bladder. There are three narrowed areas of each ureter:
- Ureteropelvic junction
- Ureteral segment
- Ureterovesical junction
Bladder is a muscular organ which holds urine. The wall of the bladder comprises of four layers:
- Adventitia
- Detrusor muscle
- lamina propria
- Urothelium – specialised transitional cell epithelium (can stretch)
Urethra Arisis from the base of the bladder and is the passageway through which urine is discharged from the body. The female urethra is much shorter (3-4cm) than the male urethra (18+cm)
Renal Physiology
- Regulation of plasma ionic composition
- Regulation of plasma volume
- Regulation of plasma osmolarity
- Regulation of plasma hydrogen ion concentration (pH)
- Removal of metabolic waste products and foreign substance from the plasma
Classification
KDIGO Staging Criteria
- Stage 1: Serum creatinine 1.5–1.9 times baseline OR >= 0.3 mg/dL (26.5 umol/L) increase; Urine output < 0.5 mL/kg/hr for 6–12 hours.
- Stage 2: Serum creatinine 2.0–2.9 times baseline; Urine output < 0.5 mL/kg/hr for >= 12 hours.
- Stage 3: Serum creatinine 3.0 times baseline OR increase to >= 4.0 mg/dL (353.6 umol/L) OR initiation of Renal Replacement Therapy (RRT); Urine output < 0.3 mL/kg/hr for >= 24 hours OR anuria for >= 12 hours.
Anatomical / Etiological Classification
- Prerenal Azotemia (~40–55%): Renal hypoperfusion without structural parenchymal damage.
- Intrinsic / Intrarenal AKI (~35–40%): Structural damage to the renal parenchyma (tubules, interstitium, glomeruli, or renal vasculature).
- Postrenal AKI (~5–10%): Acute urinary tract obstruction downstream of the renal pelvis.
Prerenal azotemia is functional and rapidly reversible upon restoring renal perfusion; if hypoperfusion persists, it transitions into structural Intrinsic AKI (Ischemic Acute Tubular Necrosis).
Aetiology
The aetiology of acute kidney injury can be simply divided into pre-renal, renal and post renal causes.
Pre-renal – Sepsis and hypotension:
- Severe sepsis
- Haemorrhage
- Dehydration
- Cardiac failure
- Liver failure
- Renovascular insult
Intrarenal
- Toxicity
- Parenchymal kidney disease
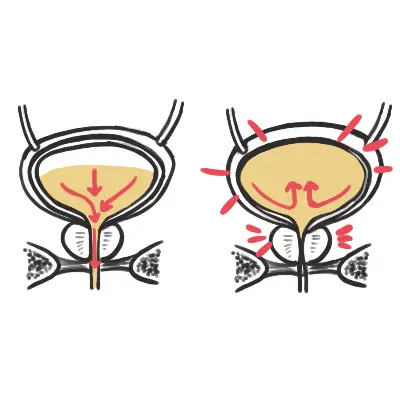
Post renal Obstruction
- Bladder outflow
- Stones
- Tumour
- Surgical ligation of ureters
- Extrinsic compression (lymph nodes)
- Retroperitoneal fibrosis
Clinical Manifestations
Fluid & Electrolyte Disturbances
- Fluid Overload: Peripheral edema, sacral edema, pulmonary congestion/edema, jugular venous distension, hypertension.
- Hyperkalemia: Life-threatening muscle weakness, paresthesias, cardiac conduction delays, and arrhythmias (peaked T waves, QRS widening, sine wave).
- Metabolic Acidosis: High anion gap metabolic acidosis due to failure of acid excretion (H+) and impaired bicarbonate reabsorption; presents with Kussmaul respiration.
- Hyperphosphatemia & Hypocalcemia: Inability to excrete phosphate; phosphate binds serum calcium causing symptomatic hypocalcemia (tetany, Trousseau/Chvostek signs).
Systemic Uraemic Manifestations
- Neurological: Encephalopathy, confusion, asterixis (flapping tremor), seizures, lethargy, somnolence, coma.
- Cardiovascular & Respiratory: Uremic pericarditis (pericardial friction rub), pleuritis, Kussmaul breathing.
- Gastrointestinal: Anorexia, nausea, vomiting, uremic fetor (ammoniacal breath odor), gastrointestinal mucosal bleeding.
- Hematological: Platelet dysfunction (impaired aggregation via uremic toxins) leading to mucosal bleeding and easy bruising despite normal platelet count.
Etiology-Specific Manifestations
- Prerenal: Thirst, orthostatic hypotension, dry mucous membranes, delayed capillary refill, history of fluid loss.
- Acute Interstitial Nephritis (AIN): Classic triad (present in < 30%): fever, maculopapular rash, and peripheral eosinophilia; history of new drug exposure.
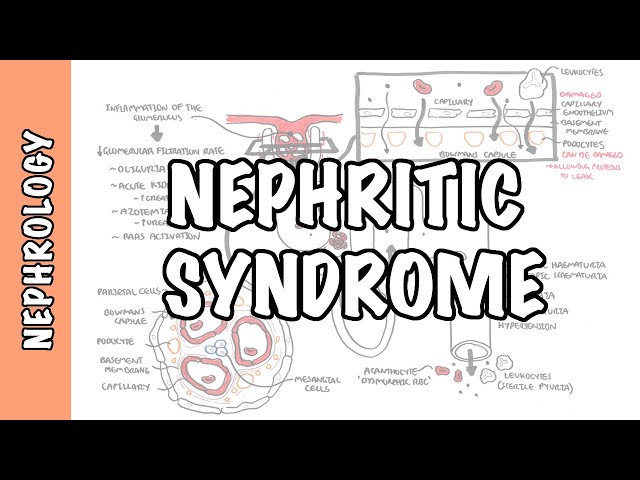
- Glomerulonephritis: Gross hematuria (“cola-colored urine”), hypertension, periorbital edema.
- Postrenal: Suprapubic pain/fullness, severe flank/colicky pain, palpable bladder, fluctuating urine output (alternating oliguria and polyuria).
REMEMBER: Asterixis (flapping tremor) and a pericardial friction rub are critical red-flag signs of advanced uremia that require emergency initiation of dialysis.
Investigations
Urinalysis & Microscopy (Crucial Diagnostic Tool)
- Prerenal: Bland sediment or transparent hyaline casts.
- Acute Tubular Necrosis (ATN): Muddy brown granular casts and renal tubular epithelial cells.
- Acute Interstitial Nephritis (AIN): WBC casts, pyuria, and urine eosinophils (Hansel stain).
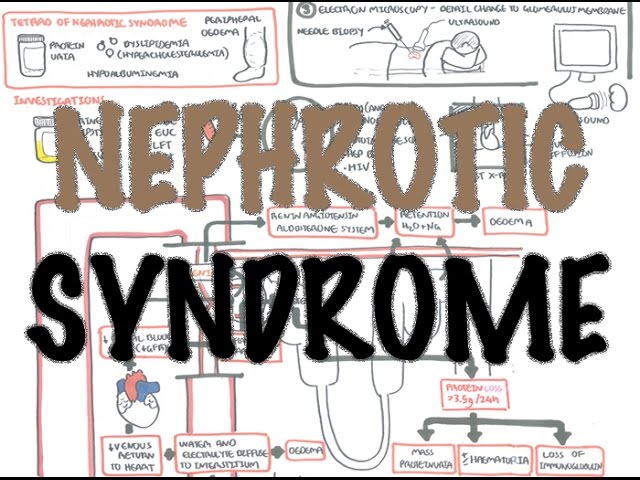
- Acute Glomerulonephritis: Dysmorphic RBCs, RBC casts, and heavy proteinuria.
- Postrenal: Normal/bland sediment, microscopic hematuria, or pyuria (if infection present).
Bloods
- FBC, EUC, LFTs
- Clotting profile
- Group and save – if anaemia
- CRP/ESR
- CK – rhabdomyolysis?
- Blood culture
- Arterial blood gas
- CMP
Percuss the bladder and perform bladder ultrasound in case the reason for oliguria is bladder in origin.
Screening for nephritis/nephrotic syndromes
- Anti-ANA
- ANCA
- Anti-GBM
- Anti-streptolysin O tites
- Protein electrophoresis
- Immunoglobuins (IgG, IgA and IgM
- Rheumatoid factor
- Viral serology – HIV, HBV, HCV
- Antiphospholipid syndrome
Imaging
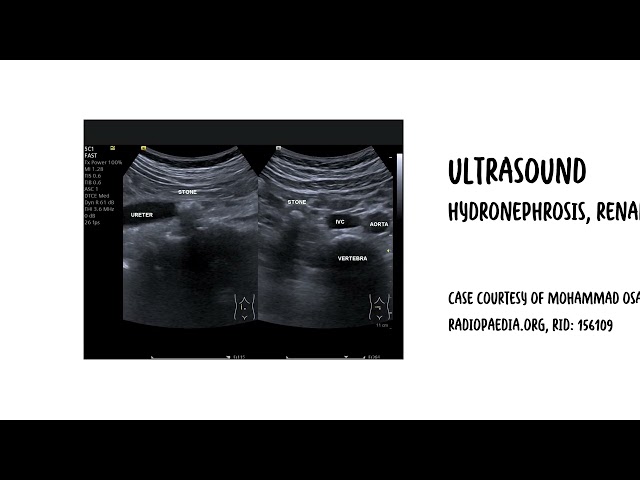
- Renal Ultrasound (First-Line Imaging): Evaluates kidney size, echogenicity, and rules out urinary tract obstruction (hydronephrosis).
- Bladder Scan & Post-Void Residual (PVR): Rapid evaluation for urinary retention / bladder outlet obstruction (PVR > 200 mL suggests obstruction).
- Renal Biopsy: Gold standard for diagnosing intrinsic AKI when etiology remains unclear (especially if glomerulonephritis, vasculitis, or AIN is suspected).
Treatment
General
- Discontinue Nephrotoxins: Stop NSAIDs, ACEi/ARBs, aminoglycosides, vancomycin, and hold iodinated radiocontrast.
- Dose Adjustment: Adjust all renally cleared medications according to estimated GFR/creatinine clearance.
- Hemodynamic Stabilization: Maintain mean arterial pressure (MAP >= 65 mmHg) using IV fluids or vasopressors (Norepinephrine first-line in septic shock).
Subtype-Specific Management
- Prerenal Azotemia
- Volume resuscitation with isotonic crystalloids (e.g., Normal Saline or Plasmalyte) for hypovolemia
- Optimize cardiac function in heart failure.
- Acute Tubular Necrosis (ATN)
- Supportive care; maintain euvolemia, manage electrolytes, avoid further insults (no evidence supports loop diuretics or “renal-dose” dopamine to convert oliguric to non-oliguric ATN).
- Acute Interstitial Nephritis (AIN)
- Discontinue culprit drug immediately
- Consider a short course of oral Systemic Corticosteroids (e.g., Prednisone 1 mg/kg/day) if no improvement after drug cessation.
- Glomerulonephritis / Vasculitis
- High-dose corticosteroids
- Cyclophosphamide OR rituximab OR
- Plasma exchange (plasmapheresis).
- Postrenal Obstruction
- Urgent urinary decompression via urethral Foley catheter, suprapubic catheter, or percutaneous nephrostomy tubes / ureteral stents.
Loop diuretics (Furosemide) help manage fluid overload in AKI, but they do NOT improve mortality, recover renal function, or decrease the need for dialysis in ATN.
Treat complications
- Hyperkalaemia
Hyperkalaemia can induce cardiac dysrhythmias with the following ECG changes: Peak T waves (tenting), flattening of P waves and prolonged PR interval
- Pulmonary Oedema
- Hyperphosphataemia
- Dietary restriction of phosphate
- PO4 removal through dialysis or haemofiltration.
- Oral phosphate binder (calcium carbonate)
- Hypocalcaemia
- Calcium is supplemented orally
In rhabdomyolysis, Ca2+ can precipitate in injured muscle, causing necrosis and ischaemic contractures—resist the administration of Ca2+ unless symptomatic hypocalcaemia.
- Hypomagnesaemia
- Magnesium supplement
- Anaemia – Bleeding?
- Infections – Antibiotics
Side note Sepsis is an important cause of morbidity and mortality in AKI (75% mortality if AKI + sepsis).
| Indications for Dialysis (AEIOU) |
| Acidosis |
| Electrolytes – refractory hyperkalaemia |
| Ingestions/intoxication – Barbiturates, lithium, alcohol, salicylates, theophyline |
| Overload – Pulmonary oedema |
| Uraemia Complications – pericarditis, refractory pulmonary oedema and encephalopathy |
Complication and Prognosis
Complications
- Hyperkalemia: Cardiac arrest from lethal arrhythmias.
- Acute Pulmonary Edema
- Uremic Complications
- Uremic pericarditis (risk of cardiac tamponade)
- Encephalopathy
- Eevere bleeding diathesis.
- Infections: Leading cause of death in AKI (~50–70% of fatalities); secondary to uremia-induced immune dysfunction and invasive lines.
- Overall in-hospital mortality is ~20%, rising to > 50% in ICU patients requiring renal replacement therapy.
- AKI is a major independent driver of chronic kidney disease; patients experiencing even a single episode of resolved AKI have an 8-fold increased risk of developing CKD and a 3-fold increased risk of end-stage renal disease (ESRD).
- Serum creatinine and urine protein should be re-evaluated at 3 months post-AKI to assess for recovery, persistence (AKD), or transition to CKD.
Hyperkalaemia can induce cardiac dysrhythmias with the following ECG changes: Peak T waves (tenting) → flattening of P waves and prolonged PR interval
Infection—not uremia itself—is the leading cause of death in patients suffering from acute kidney injury
References
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2(1):1-138.
- Bellomo R, Kellum JA, Ronco C. Acute kidney injury. Lancet. 2012;380(9843):756-766. doi:10.1016/S0140-6736(11)61454-2
- Ostermann M, Zarbock A, Goldstein S, et al. Recommendations on Acute Kidney Injury Biomarkers From the Acute Disease Quality Initiative Consensus Conference: A Consensus Statement. JAMA Netw Open. 2020;3(10):e2019209. doi:10.1001/jamanetworkopen.2020.19209






Members only discussions coming soon…