Aneurysm

An aneurysm is an abnormal localised dilatation of a blood vessel with at least 50% increase in diameter compared to its normal diameter. It is seen more often in arteries compared to veins. Aneurysms are usually asymptomatic until they are very large or they rupture. A ruptured aneurysm can cause massive bleeding and death.1
Aneurysm: an artery that has enlarged to greater than 1.5 times the expected diameter.
True Aneurysm: The aneurysm is bound by all three layers of the vessel wall (intima, media and adventitia). The wall may be attenuated.
False Aneurysm: Occurs when a blood vessel wall is injured, and the blood is contained by the surrounding tissues creating an apparent dilatation of vessel.
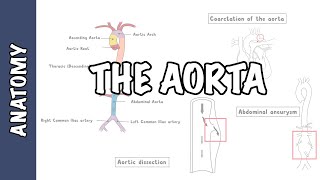
Aortic dissection: occurs when a tear in the tunica intima of the aorta causes blood to flow between the layers of the wall of the aorta, forcing the layers apart.
True Aneurysm – involves all three layers of the vessel wall; it can be divided into:
Fusiform: circumferential (symmetrical) bulging
Saccular (Berry aneurysm): focal (asymmetrical) outpouching
False Aneurysms (pseudoaneurysm) – collection of blood in the outer layer only, which communicates with the lumen.
True Aneurysms
False Aneurysms
True aneurysm
Endothelial injury and inflammation
↓
Increased matrix metalloproteinases and proteolytic enzyme activity
↓
Elastin and collagen degradation and smooth muscle apoptosis
↓
Tunica media thinning
↓
Loss of strength and elasticity
↓
Progressive wall dilatation
↓
Increased radius causing increased wall tension (Law of Laplace)
↓
Further expansion and true aneurysm formation
False aneurysm
Direct arterial wall injury
↓
Full thickness wall disruption
↓
Blood escapes into surrounding tissue
↓
Contained haematoma formation
↓
Fibrous capsule development
↓
Persistent arterial communication
↓
Pulsatile expanding sac
↓
False (pseudo) aneurysm
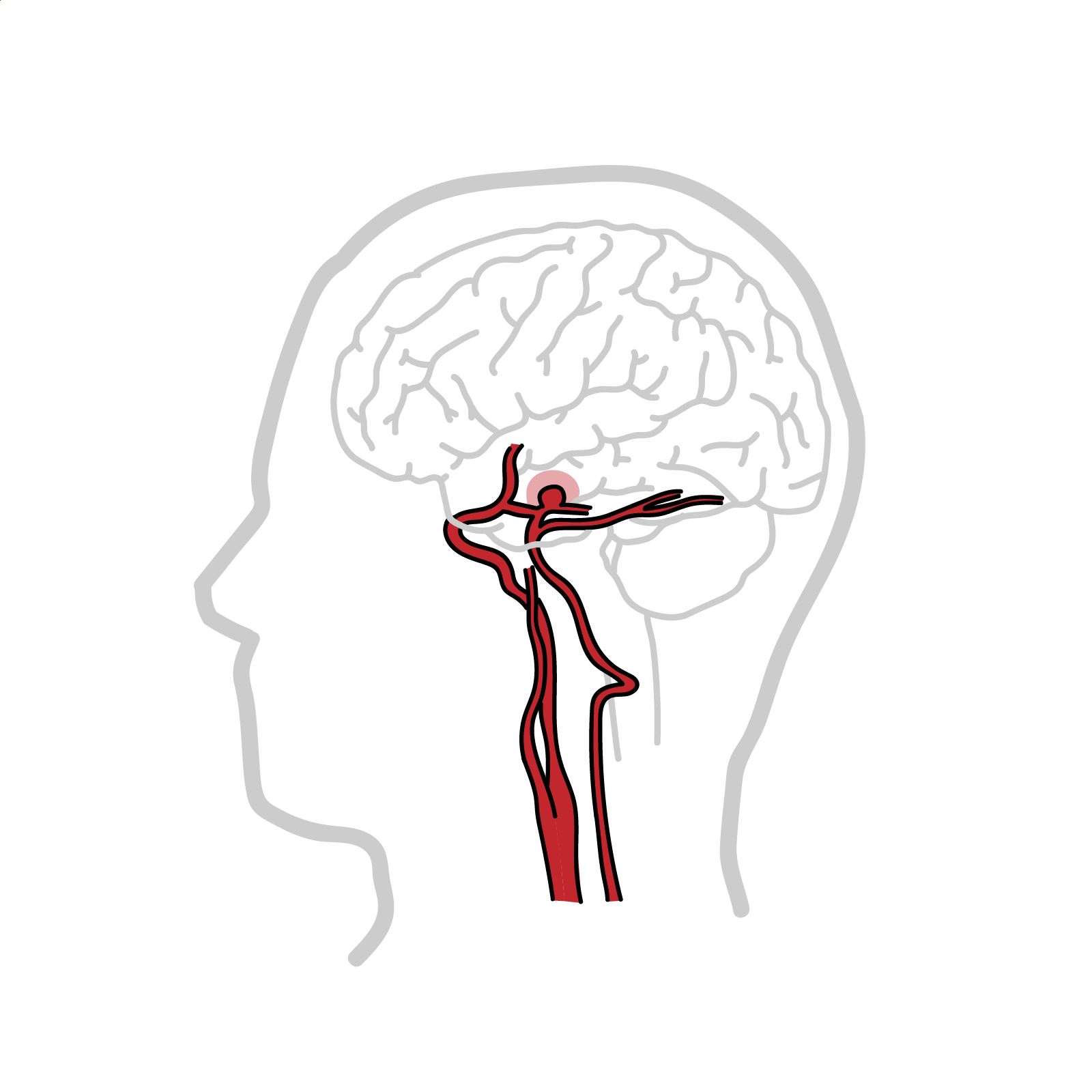
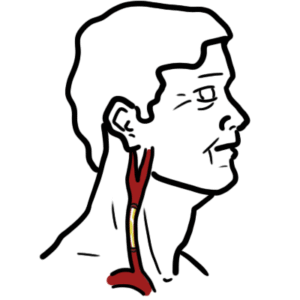
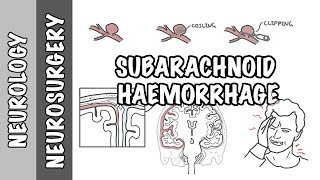
A cerebral aneurysm is a localised dilatation of an intracranial artery, usually occurring at branching points. Most common location is the anterior communicating artery, followed by the posterior communicating artery.
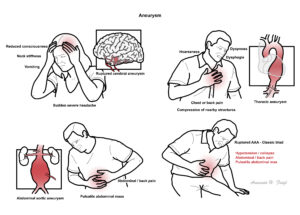
These arteries are located within the subarachnoid space, so a cerebral aneurysm rupture will result in a subarachnoid haemorrhage. A ruptured aneurysm will present with a “thunderclap” headache, vomiting, reduced consciousness, neck stiffness and photophobia.
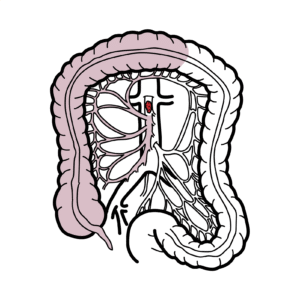
Not usually associated with atherosclerosis. These aneurysms are mainly asymptomatic, unless there is compression of local structures, which can cause chest or back pain, dyspnoea, hoarseness or dysphagia. Main diagnostic finding is a widened mediastinum on a chest x-ray, CT or MRI. Rupture has high mortality and is rare without prior symptoms. 4
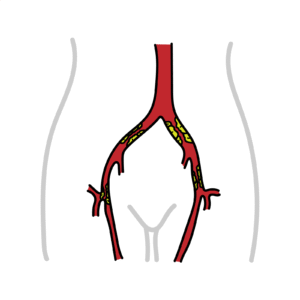
For more Information AAA
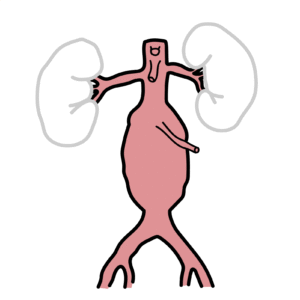
Classic ruptured AAA triad: Hypotension/collapse, back/abdominal pain, Palpable/pulsatile abdominal mass.
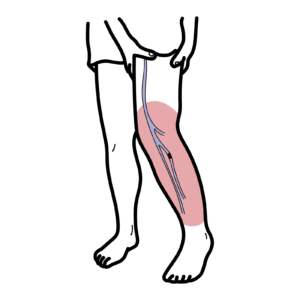
Aortic dilatation of 3cm or more, mainly linked with atherosclerosis. Most AAAs are infrarenal, meaning they are located below the renal arteries. Some may extend to involve the origins of the common iliac arteries. AAA is also associated with other peripheral aneurysms, such as popliteal. Majority are asymptomatic and are detected incidentally but they can present with abdominal, back or flank pain, or as a pulsatile abdominal mass. Risk of rupture and mortality increases with the diameter of the aneurysm. 5
AAA greater then 5.5cm in diameter need some for of intervention.
Classic triad of ruptured AAA congenital: Hypotension/collapse, back/abdominal pain, Palpable/pulsatile abdominal mass.












Discussion