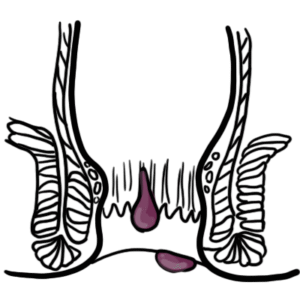
Fistula-In-Ano, also referred to as “Anorectal fistula”, is an abnormal tunnel between the anal canal (hollow viscus) and the surface of the body. Over 90% are attributed to prior anorectal abscess. It may occur in the presence of Crohn’s Disease and has an association with obesity and diabetes. Patients experience intermittent rectal pain, pruritus and malodorous drainage.1
Definition
Fistula: An abnormal connection of two epithelial surfaces Fistula in Ano: abnormal connection of the anorectal epithelial surface to the perineal skin Sinus: Granulating track leading from a source of infection to a surface
Crohn Disease is associated with ano-rectal disease.
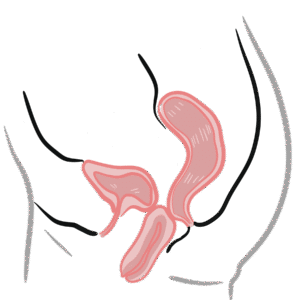
Anal canal – channel connecting the rectum to the anus, located within the anal triangle of the perineum, between the two ischioanal fossae
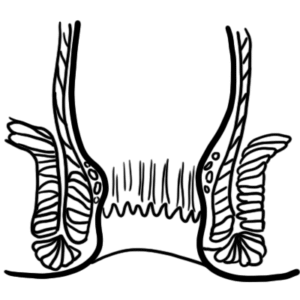
Anal Sphincters
Internal sphincter
Involuntary control – continuation of circular fibers of the colon so it receives autonomic supply
Surrounds upper 3/4 of anal canal
External sphincter
Voluntary control
Surrounds entire length of anal canal
Consists of three parts – subcutaneous, superficial and deep
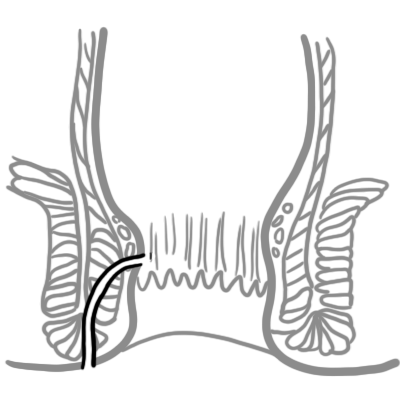
Intersphincteric plane
Between external sphincter muscle laterally and the longitudinal muscle (inner sphincteric muscle) medially
Contains anal glands
Can be opened up surgically to provide access for operations on the sphincter muscles
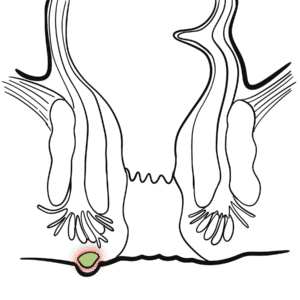
Anal glands
Apocrine glands
Occasionally infected and act as a source of anal fistula
Dentate (pectinate) line
Junction of the proximal and distal segments of the anal canal
Divides the anus into proximal 2/3 and distal 1/3
Situated at the middle of internal sphincter
Above Dentate line
Below Dentate line
Embryology
Hindgut (endoderm)
Proctodeum (ectoderm)
Epithelium
Columnar
Stratified squamous
Arterial supply
Superior rectal a.
Middle rectal a.Inferior rectal a.
Venous drainage
Superior rectal v.
Middle rectal v.Inferior rectal v.
Innervation
Visceral – Inferior hypogastric plexus(insensitive to pain)
Somatic – Inferior rectal nerves: branches of Pudendal nerve(sensitive to pain)
Lymph drainage
Internal iliac
Superficial inguinal
Hilton’s Line also called while line/anocutaneous line indicates lower end of the internal sphincter. Ischiorectal abscess when communicates with anal canal usually opens at or below Hilton’s line.
Aetiology and Risk factors
Anal abscess (most common)
Crohn disease
Obstetric injury
Radiation proctitis
Rectal foreign bodies
Infectious disease – Lymphogranuloma venerum and Actinomycosis
Chronic: discharge of seropurulent fluid with an identifiable punctum (opening)
Examination
The perianal skin may be excoriated and inflamed
External opening visible (may drain pus or blood on manual compression)
Internal opening identification may need a proctoscope (or sigmoidoscope if internal opening in rectum)
Palpable cord-like tract
Goodsall’s rule (law): Relates the external opening of an anal fistula to its internal opening. Fistulas can be described as anterior or posterior relating to a line drawn in the coronal plane across the anus. Anterior fistulas will have a direct track into the anal canal. Posterior fistulas will have a curved track with their in internal opening lying in the posterior midline of the anal canal. An exception to the rule are anterior fistulas lying more than 3cm from the anus, which may open in the anterior midline of the anal canal.
Vogel JD. Anorectal fistula: Clinical manifestations and diagnosis. In: Weiser M, editor. UpToDate [Internet]. [updated 2025 Oct 30; cited 2025 Nov 7]. Available from: UpToDate
Champagne BJ. Operative management of anorectal fistulas. In: Weiser M, editor. UpToDate [Internet]. [updated 2024 Aug 22; cited 2025 Nov 7]. Available from: UpToDate
Simpson JA, Banerjea A, Scholefield JH. Management of anal fistula. In: BMJ Best Practice [Internet]. 2012 [cited 2025 Nov 7]. Available from: BMJ Best Practice









Discussion