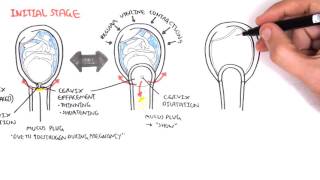
Hydatidiform Mole (Molar Pregnancy)
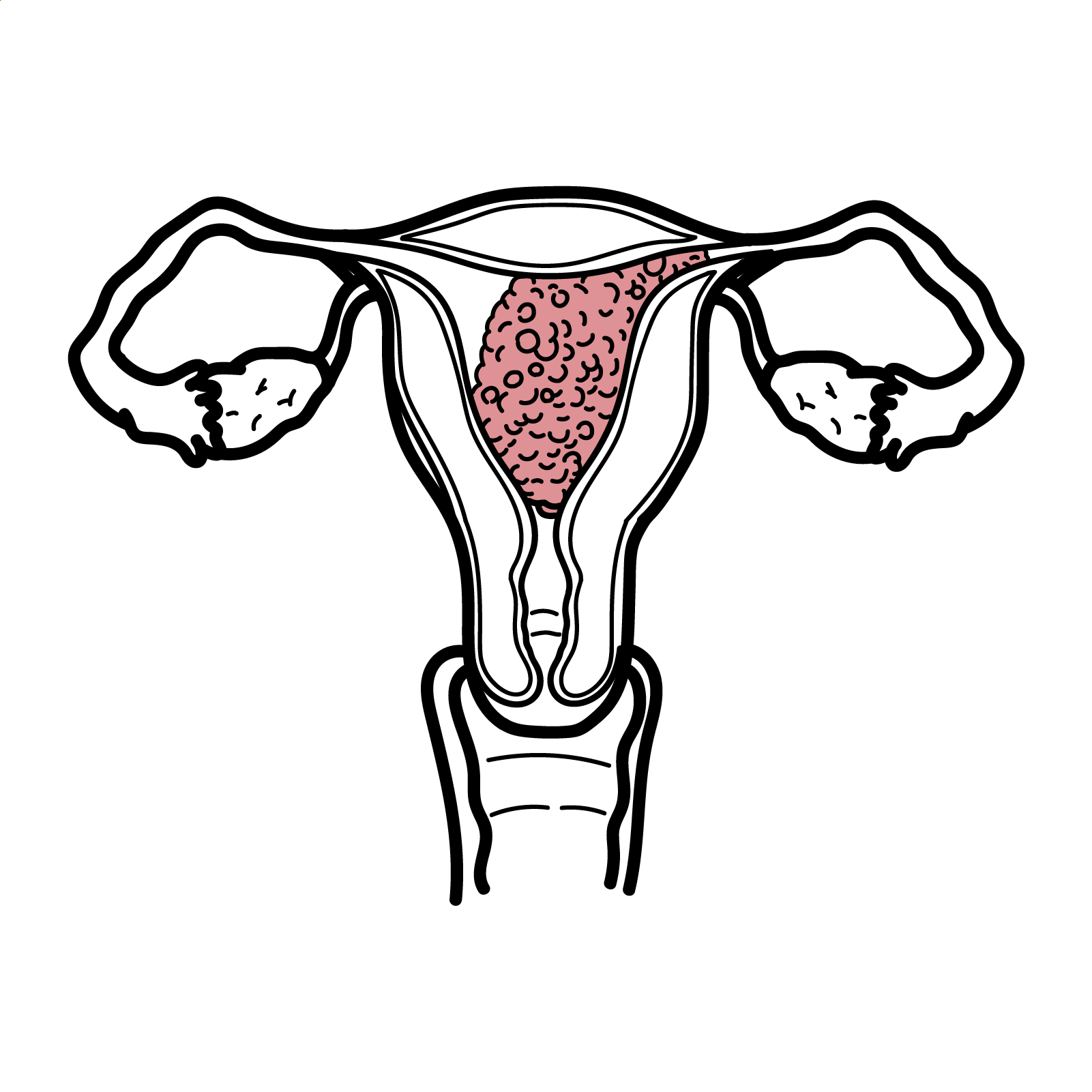

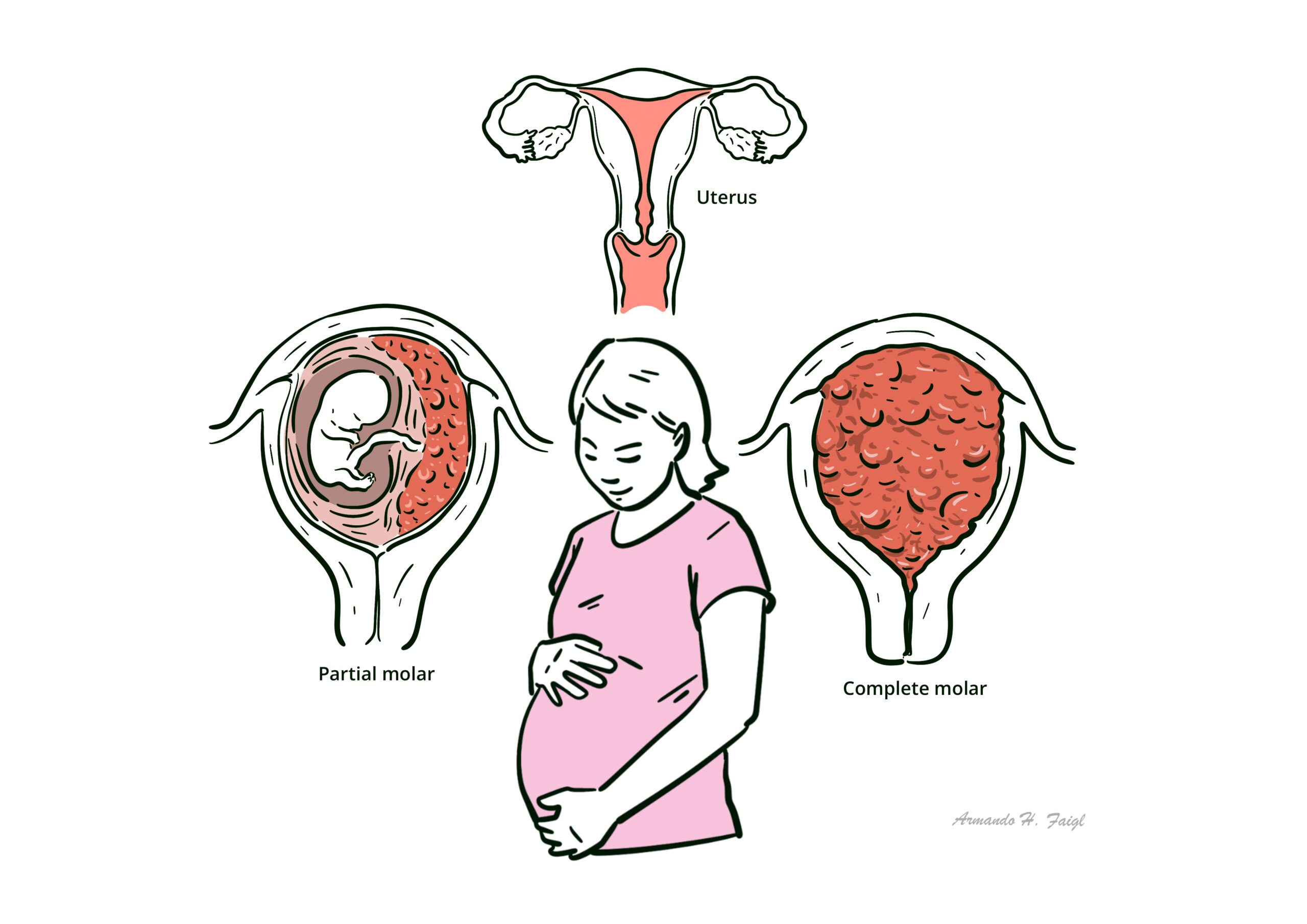
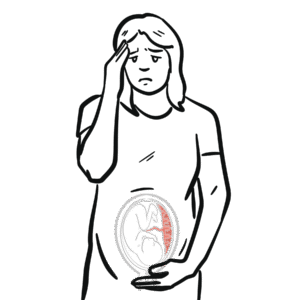
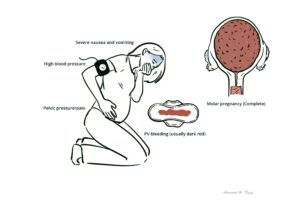
Hydatidiform moles are part of a group of diseases falling under gestational trophoblastic disease. A hydatidiform mole refers to the abnormal growth of trophoblastic cells in the placenta, resulting in edematous placental villi that form hydatidiform structures. It is classified as either partial or complete, causing either abnormal foetal development (resulting in foetal demise) or the prevention of foetal development completely, respectively. It is often identified within the first trimester of pregnancy, usually ending in miscarriage. Key features of hydatidiform moles may include first-trimester PV bleeding and severe nausea and vomiting.
Molar pregnancies are rare, affecting 1 in 1000 pregnancies in Australia, with the major risk factor being older maternal age. Molar pregnancies commonly end in miscarriage due to incompatibility with life. Early detection of a molar pregnancy reduces morbidity from uterine evacuation. Further, surveillance of B-hCG is crucial for the detection of complications such as cancer.1,2
Hydatidiform mole – An abnormal pregnancy with trophoblastic proliferation and hydropic swelling of chorionic villi, resulting in a non-viable conception.
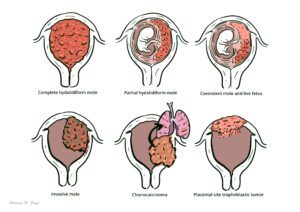
Gestational trophoblastic disease – A spectrum of pregnancy-related disorders arising from trophoblasts, including hydatidiform mole, invasive mole, choriocarcinoma, and PSTT.
Trophoblast – Placental cells (cytotrophoblasts and syncytiotrophoblasts) that normally form the chorionic villi and produce hCG.
Chorionic villi – Finger-like projections of the placenta that become swollen, oedematous, and avascular in hydatidiform mole.
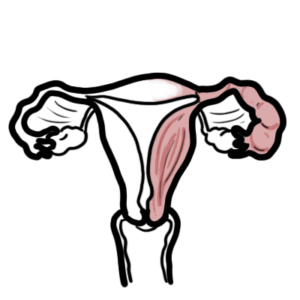
In normal pregnancy, fertilisation refers to the fusion of one haploid maternal gamete (oocyte) and one haploid paternal gamete (sperm), resulting in a diploid zygote containing one set of chromosomes from each parent. After fertilisation, the zygote continues to proliferate to form a solid ball of cells. This then hollows out to form a blastocyst, ready to implant into the uterus. A blastocyst is one cell thick (made of trophoblasts), except on one side of the blastocyst, which has the inner cell mass (about 3-4 cells thick). The inner cell mass develops into the embryo, and the outer trophoblasts form the placenta (see image below).
The placenta produces several hormones to support the pregnancy. Notably, human chorionic gonadotropin (hCG) is produced to prevent further ovulation and to increase the production of estrogen and progesterone.3
Established risk factors for abnormal fertilisation include a previous history of molar pregnancy and advancing age. There is a 2.5- and 5-fold increased risk of molar pregnancy in mothers over the age of 35 and 40, respectively.1
Belongs to the spectrum of gestational trophoblastic disease. There are three broad groups.
Hydatidiform mole (molar pregnancy) there are two types:
| Feature | Complete Mole | Partial Mole |
| Genetic origin | Empty ovum + 1/2 sperm → 46,XX/XY paternal only | Normal ovum + 2 sperm → 69,XXX/XXY |
| Fetal tissue | Absent | Present/abnormal |
| Villous oedema | Diffuse | Focal |
| Trophoblastic proliferation | Diffuse, circumferential | Focal, mild |
| hCG levels | Very high | Mildly elevated |
| Risk of malignancy | 15–20% (higher) | 1–5% (lower) |
| Complete | Partial |
| Poorly vascularised chorionic villiHydropic swellingOedematous stromaCistern with stromal fluid | Less trophoblastic proliferationFocal distribution of proliferative areasSparse regions of oedematous villi |
Complete mole = completely paternal → empty ovum, no fetus, diffuse trophoblastic proliferation, very high hCG.
Partial mole = partly maternal → abnormal fetus present, triploidy, focal villous changes, lower hCG than complete mole.
Picture molar pregnancies as an exaggerated pregnancy: e.g., larger uterus, severe nausea and vomiting, anaemia and thyroid issues .
Very high β-hCG → may cause exaggerated pregnancy symptoms (hyperemesis gravidarum, hyperthyroidism, theca lutein cysts).
Pre-eclampsia before 20 weeks → pathognomonic for molar pregnancy until proven otherwise.
First line investigation: ultrasonography
Other investigations
Definitive (gold standard): Dilation and curretage with histopathology
“Snowstorm” or “cluster of grapes” ultrasound → hallmark of complete mole, no fetus seen.
General measures
Chemotherapy (methotrexate or actinomycin-D):
Complications
The most alarming complication of Gestational Trophoblastic Disease is Gestational Trophoblastic Neoplasia (GTN), a pregnancy-related cancerous tumour. B-Hcg surveillance as outlined above is the gold standard investigation for monitoring of GTN.
β-hCG surveillance is vital for preventing GTN. It must be measured at baseline, then weekly, until it returns to normal for 3 consecutive weeks. Then, if a complete molar pregnancy, continue monitoring monthly for 6 months.





Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.






Discussion